
Review Article | DOI: https://doi.org/10.31579/2693-2156/017
Assistant Professor, Department of Cardiac Surgery, Chittagong Medical College, Chittagong, Bangladesh
*Corresponding Author: Md. Anisuzzaman, Assistant Professor, Department of Cardiac Surgery, Chittagong Medical College, Chittagong, Bangladesh
Citation: Md. Anisuzzaman (2021). Christian N Barnard: A man who dared the first human to human heart transplant. J Thoracic Disease and Cardiothoracic Surgery, 2(1); DOI:10.31579/2693-2156/017
Copyright: © 2021 Md. Anisuzzaman, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 April 2021 | Accepted: 16 April 2021 | Published: 22 April 2021
Keywords: heart transplantation; surgical technique; cardiac surgery; immunosuppressive therapy; GSH; UCT; technical virtuosity; heart-lung machine
Heart transplant had already developed by a group of US surgeons in the early 1950s, and it was the American pioneer Norman Shumway who validated the technical feasibility in a dog model at Stanford University in 1958. This milestone in medicine was the beginning of a huge race for numerous physicians and researchers to make this operation a clinical reality. Barnard was intrigued by the idea to perform heart transplantation at Groote Schuur Hospital and therefore made it a major focus in his department in the early 1960s. While Shumway and co-workers were further refining the surgical technique in these year, based on his extensive cardio-surgical experience, Barnard was already convinced about the technical feasibility and wanted to enter this new field of cardiac surgery. To accomplish his goal, he recognized that he had to learn more about immunosuppressive therapy and therefore he spent a few months in Richmond, VA, USA, to obtain this important knowledge for postoperative care. In 1966, when Shumway and colleagues announced that they would be ready for a first human patient, Barnard moved ahead of them on 3 December 1967, and performed the world’s first human-to-human heart transplantation.
The first human heart transplant had been carried out by the South African surgeon, Christiaan Barnard at Groote Schuur Hospital (GSH) in Cape Town on December 3rd, 1967. The daring operation and the charismatic surgeon received immense public attention around the world. The patient’s progress was covered by the world’s media on an almost hourly basis. Although the patient, Mr. Louis Washkansky, died after only 18 days, Barnard soon carried out a second transplant, and this patient led an active life for almost 19 months. Remarkably, Barnard’s fifth and sixth patients lived for almost 13 and 24 years, respectively. Barnard subsequently introduced the operation of heterotopic heart transplantation in which the donor heart acted as an auxiliary pump, with some advantages in that early era. It took great courage to carry out the first heart transplant, and this is why Barnard is remembered as a pioneer in cardiac surgery [1].
Early life and education:
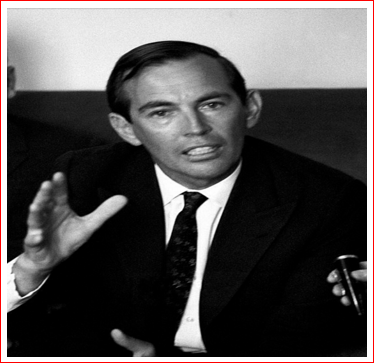
Christiaan Nethling Barnard (Figure 1) was born on 8 November 1922 and 3rd son of poor church minister in the rural town of Beaufort West in South Africa, approximately 300 miles from Cape Town. After attending the local high school and matriculating with a first-class degree in 1940, Barnard did well enough to gain entry to study medicine at the University of Cape Town (UCT), where he was financially dependent on two scholarships he had been awarded. If he failed an examination, he would lose the scholarships and would no longer be able to pursue his goal of becoming a doctor. He graduated at the end of 1946 and after internships in Cape Town, he married and joined a general practice in a small town about an hour’s drive inland from Cape Town. Then he returned to the Cape Town area to study for higher surgical examinations and joined at the local infectious disease hospital. This led to further appointments, first in medicine and then in surgery, at GSH, the major UCT teaching hospital. In 1953, he was awarded the master and doctoral degree in medicine, before started working as a registrar at the Department of Surgery at the GSH under the guidance of Prof. J. Louw. During this period, he carried out some very innovative research in a canine model of intestinal atresia in neonates [2].
He was then offered a scholarship by Prof. John Brock of GSH to gain surgical experience at the University of Minnesota in Minneapolis under the tutorship of the legendary Professor Owen Wangensteen in 1956. It was there that he was first exposed to the very new field of open heart surgery, the University hospital in Minneapolis being only one of a handful of centers in the world where this form of surgery was being carried out. Barnard immediately saw the potential of the heart-lung machine (pump-oxygenator) and, under the direction of C Walton Lillehei (perhaps the most important of the early open heart surgery pioneers) and his colleague Richard Varco, steadily gained experience. Prof. Lillehei quickly noticed the enormous will and passion this young South African doctor had and offered him a permanent job in his team. However, Barnard rejected this generous offer as he felt he had to return to South Africa [1,2].
In 1958 he received a Master of Science in Surgery for a thesis titled “The aortic valve- problems in the fabrication and testing of a prosthetic valve”. The same year he was awarded Doctor of Philosophy degree for the dissertation titled “The etiology of congenital intestinal atresia”.
After 30 months in the USA, he returned to UCT with a pump oxygenator in 1958. He immediately initiated an open heart surgery program at GSH, which was associated with excellent results and gained him a good reputation from those who followed his progress [3,4]. Among his achievements was to become the first surgeon to correct Ebstein’s anomaly [5], and to have probably the world’s best results from the correction of Fallot’s tetralogy [6]. He also designed and implanted a prosthetic valve that was successful for that era [7].
Probably the most important thing for Barnard was the presence in the medical school of a strong department of experimental surgery, founded with remarkably perspicacity some 30 years earlier. In 1958, Barnard was appointed as its head (Director of Surgical Research), and he began to develop an ambitious program of open heart surgery. He was egocentric, hardworking, clever, ambitious, brash, and somewhat arrogant; he functioned on the principle that anything others could do he could do at least as well. In 1960, he flew to Moscow in order to meet Vladimir P Demikhov, a top expert on organ transplants. When a report appeared that a Russian surgeon had grafted a second head on to a dog, Barnard immediately did the same thing, a grotesque accomplishment he proudly displayed to those who were in the medical school at the time. There was no clear purpose to this other than to show his technical virtuosity. In 1961, he was appointed Head of the Division of Cardiothoracic Surgery at the teaching hospitals of the University of Cape Town.
In the early 1960s, by which time heart surgery could correct most congenital heart defects and valve disease (but not yet coronary artery disease), he began to consider the future of his career. He considered that heart transplant would be required if end stage heart failure patients were to be helped [1].
Ground works for heart transplant:
Barnard and his younger brother, Marius, who was also a cardiac surgeon at GSH, began by gaining experience of the operation of orthotopic heart transplantation in dogs [8]. He used an operative technique first described by Russel Brock and a junior colleague in London in 1959, but extensively developed and investigated by Norman Shumway and his research team at Stanford University in the USA [9].
At first, the main aim of Barnard was to perfect the surgical technique. Then he took experience in immunosuppressive therapy in patients with kidney transplants. For this he attached himself for three months to the transplant program headed by David Hume in Richmond, Virginia in the summer of 1966. There he also gained more experience of experimental heart transplant in the laboratory of Richard Lower, who had trained with Shumway, but had subsequently been recruited to Richmond by Hume. While Shumway was working with surgical technique, Barnard was already convinced about the technical feasibility and wanted to enter this new field of cardiac surgery.
In 1966, when he returned from his stay in Richmond, Shumway and colleagues announced at several international conferences that they would be ready for a first human patient. On November 20, 1967, Dr Shumway finally announced that it was an appropriate time to proceed with human cardiac transplantation once a suitable donor and recipient could be found. This announcement received news coverage around the world. The following day, the South African Cape Times announced that a team at Groote Schuur Hospital was on standby to perform a heart transplant [10].
When Barnard returned to GSH, carried out a single kidney transplant (second kidney transplant in South Africa) on a patient who lived for 20 years. Then Barnard felt ready to carry out a first heart transplant. He asked the professor of cardiology, Velva Schrire, a superb clinician, to select a patient who might benefit from the procedure. Professor Schrire believed that selection of non-white recipient or donor might be misinterpreted by the political critics of South Africa as experimenting on the non-white population. They therefore agreed that both recipient and donor should be Caucasian (white).
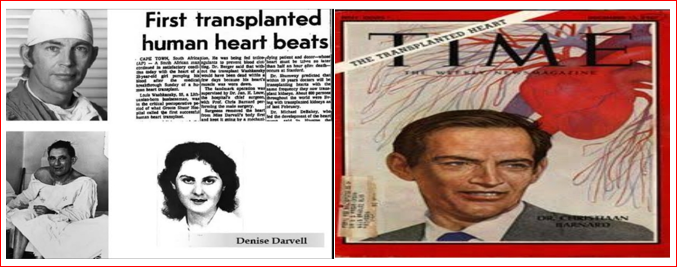
Schrire identified Louis Washkansky, a 53-year-old diabetic, who was bedridden in hospital in severe cardiac failure from ischemic heart disease [11]. Washkansky accepted the opportunity as he knew he had no alternative if he wanted to stay alive. The surgical team then waited for a suitable donor. In the afternoon of Saturday, 2 December 1967, Denise Darvall, a 25-year-old woman, was brought to GSH having suffered a severe brain injury as a result of a road traffic accident [12]. Within hours, she was certified brain-dead by the hospital neurosurgeons, and her father gave his consent for her heart and kidneys to be used for transplantation.
The first heart transplant:
In the early hours of 3rd December, 1967, the recipient and donor were taken to the operating room suite. In that era, the law in South Africa simply stated that a patient was considered dead when he/she was declared dead by a physician. But Barnard decided to wait further for the heart to stop beating before he remove it. He therefore disconnected the ventilator, and waited until the EKG indicated no cardiac output. This took approximately six minutes.
The chest was then opened quickly by splitting the sternum. The heart was blue and not beating. The surgical team connected the donor to a heart-lung machine, and circulated cold oxygenated blood through her body, with the aim of reducing the metabolism of the heart while it was transplanted. The heart was rapidly cooled to a low temperature, helping to protect it from further ischemic injury during transplantation. The donor heart was excised in such a way that the donor heart-lung machine would continue to perfuse it with cooled oxygenated blood while it was carried into the adjacent recipient operating room. Thus, the heart continued to be protected from injury.
This approach is rarely followed today when a beating donor heart is simply cooled to a very low temperature by perfusing it with a cold preservation solution, then excised, and covered in ice or cold saline. However, the continuous perfusion of the donor heart with oxygenated blood in Mr. Waskansky’s case may have been important as Barnard had allowed the heart to suffer an insult and possibly injury while it stopped beating, which is much less commonly allowed today. Although Barnard and two of his colleagues, including his brother, Marius, had carried out a relatively large number of heart transplants in dogs, Chris’s two major assistants on the day of this first clinical operation had never seen a heart transplant in their lives before-not even in a dog.
Louis Washkansky’s heart was then removed from his chest. Chris told that, “and for the first time in my life, I stared into an empty chest.” (Although by this stage of his career, he had carried out hundreds, if not thousands, of heart operations, he had never before looked into a human chest and seen no heart.) “At that moment, the full impact of what I was attempting became abundantly clear to me.” The donor heart was quickly sewn in place without difficulty.
Mr. Washkansky’s heart had become dilated over the years and failed to cope with the blood to pump around the body. It was therefore much larger than a normal heart. Denise Darvall’s heart was much smaller than even a healthy man’s heart, and so it looked tiny in the large space left by Mr. Washkansky’s heart. Barnard Looked at it and wondered whether it was too small to support the circulation in such a relatively big man. This observation must have been very disturbing to him, but he could do nothing about it now.
Once Barnard had completed the transplant, he allowed the blood from the recipient’s heart-lung machine to perfuse through the new heart. By warming the blood as it passed through the heart-lung machine, he also raised the patient’s body temperature back to normal. The surgical team waited for the heart to beat, but for some minutes it refused to do so (although it was fibrillating). Barnard became increasingly worried that the heart muscle had been severely damaged when he had disconnected donor’s oxygen supply. He then electrically defibrillated the heart, and at last it began to contract normally, but weakly, and would not take over the circulation.
Barnard tried twice to wean the patient from heart-lung machine, but the heart was not beating strongly enough to maintain an adequate blood pressure. He then allowed more time for the donor heart to gain strength and keep in pump. Steadily the contraction became stronger. At the third attempt to disconnect from pump, the blood pressure kept rising. Barnard told, “Naturally, I felt a great sense of relief”. The heart-lung machine could now be switched off, and the chest closed. The operation had been successful. From ‘skin to skin’, it had taken almost 5 h. It was 6.15a.m. Chris reached across the operating table and shook his chief assistant’s gloved hand. When he was satisfied the heart was beating well and the patient would recover, Barnard left his colleagues to close Mr. Washkansky’s chest [1].
Barnard had not even informed the chairman of the surgery department. He said, “I didn’t think it was necessary”, suggesting that he did not realize the impact the operation would make worldwide. He only telephoned an old friend of student life, member of the Executive Committee in charge of Hospital and Health Affairs in the Cape Provincial Administration [13]. This politician immediately recognized the significance of the transplant and by the way informed the Prime Minister of South Africa within 30 minutes. The politicians had immediately realized its potential impact on the world. It could put South Africa on the medical map. There were no photographers at the first transplant. Barnard told, “not because we wanted to keep them away, but because we honestly did not think it was a big deal.” How wrong could he be? Within hours, the hospital received an offer of US$1 million for a photograph of the donor heart being placed into the chest of Mr. Washkansky on the operating table, but of course, no photograph had been taken. Furthermore, when he left the operating room, Barnard discarded his surgical gloves in the trash can as usual, only to learn a few days later that a newspaper was offering to purchase them for US$25000 [1].
Mr. Washkansky settled safely in the intensive care room, Barnard drove home. It was an hour later when phone calls came from all over the world. Public interest was so great that the entire team was called back into the hospital that afternoon to be photographed. It may perhaps be difficult to explain what is meant by ‘media attention’. Photographers and Journalists flew in from all over the world and swarmed over Groote Schuur Hospital. Television and radio services worldwide provided updates and bulletins on Mr. Waskansky’s progress throughout the day. On the front page of several local newspapers, a photo showed Louis Washkansky, and was transmitted around the world within twenty-four hours (Figure 2A, Figure 2B). Indeed, the whole world watched the patient’s progress.
After the first week, Mr. Washkansky began to feel tired and less well. His condition began to deteriorate after 12 days and developed radiographic infiltrates in the lungs. In retrospect, it is clear that his recovery was impaired by allowing him to have too many visitors and give too many interviews to the media. David Hume had described as “transplant lung”, a reaction in the lungs in response to rejection in the transplanted organ (that was later disproved).
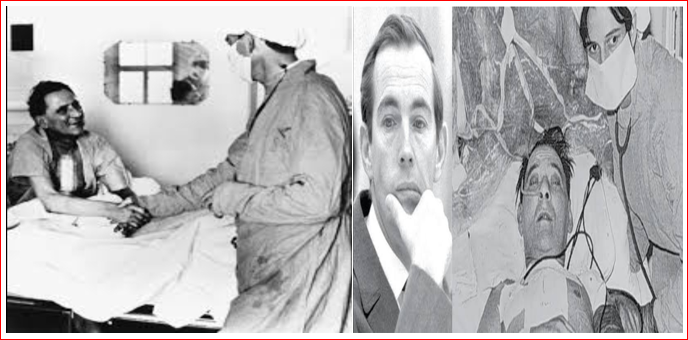
Influenced from what he had learnt in Richmond, Barnard unfortunately increased the patient’s immunosuppressive therapy until it became clear that the patient had pneumonia. Despite intensive antibiotic therapy, Mr. Washkansky deteriorated rapidly and died in the early hours of Thursday, 21st December, 18 days after the transplant (Fig-3A, Fig-3B). Barnard was devastated by this sad outcome. Autopsy showed no features of rejection and confirmed that death had resulted from pneumonia. By inspecting the suture lines, Professor Thompson ascertained that Barnard had performed the operation faultlessly [14].
After the disappointment of Mr. Waskansky’s transplant, Barnard soon added in the list, Mr. Philip Blaiberg, retired dental surgeon with similar terminal cardiac failure. A donor became available on 2nd January, 1968, and the operation proceeded satisfactorily. He was discharged on 74th post-operative day, and lived active life for 19 months [15], eventually died of chronic rejection.
Barnard’s 3rd patient, Petrus Smith, lived for 20 months, when patients of other centers worldwide died within a few days or weeks. Remarkably, his fifth patient lived for almost 13 years, the sixth one for more than 23 years [16].
Barnard steadily distracted from his work, as he was seemingly always willing to accept any invitation to speak anywhere in the world. The heart surgery program at GSH increasingly led by his very competent younger brother, Marius, but Barnard’s day-to-day leadership and vision were obviously missed. After experiencing some early graft failures, in 1975, set his junior colleague Jacques Losman to design heterotopic heart transplant (as an auxiliary heart) [17]. Heterotopic heart transplant continued at GSH for several years, but when cyclosporine added to minimize rejection, Barnard’s unit reverted to orthotopic heart transplant [18]. Barnard’s junior research colleague, Winston Wicomb had introduced hypothermic perfusion of donor heart as a means of protecting the heart during transportation to GSH, enabling for the first time hearts to be procured at centers far distant from Cape Town [19]. In addition, Barnard’s junior surgical colleague, Dimitri Novitzky, was carrying out his groundbreaking studies on the pathophysiology of brain death and the beneficial effects of thyroid hormone therapy on donor heart function, a therapy that is now used worldwide [20].
Barnard took early retirement form GSH in 1983, at the age of 61 and spent more time on the many other interest like public speaking and writing [21]. He wrote two autobiographies [22], four novels, and a book in which he discussed South Africa’s political problems and his suggestions for resolving them [23]. In 1986, he accepted an invitation to help surgeons in Oklahoma City establish a heart transplantation program. Although he did not participate in actual surgery and patients care, with his advice and public relations activities, did much to establish a successful program [1]. He had by this time become very interested in anti-aging research, and his reputation suffered in 1986 when he promoted Glycel, an expensive anti-aging skin cream, whose approval was withdrawn by the United States Food and Drug Administration soon thereafter. He also spent time as a research adviser to the Clinique la Prairie, in Switzerland, where the controversial “rejuvenation therapy” was practiced. Barnard divided the remainder of his years between Austria, where he established the Christiaan Barnard Foundation, dedicated to helping underprivileged children throughout the world, and his game farm in Beaufort West, South Africa.
His personal life was chequered. He was married and divorced three times, having two children with each wife. Complicated by ill health and loneliness, his last few months were the most miserable of his life. He died suddenly due to severe asthma attack while on holiday in Paphos, Cyprus on 2nd September 2001, at the age of 78 [1].
Today, when heart transplantation has become a relatively routine and common procedure, we may be inclined to underestimate Bernard’s immense confidence and courage in undertaking the first operation. By any standard, it was a monumental step to take. Maybe the few other surgeons who were planning heart transplants at that time, did not have the same courage, particularly those in countries where litigations against doctors was more common. However, he will also be remembered as a man who enjoyed life to the full, and employed his personality, sense of humor, and articulacy to inform and entertain thousands through his public lectures and appearances on television. Unfortunately, his personal life and public behaviour distracted his role in medical profession, and the colleagues, who perceived him as something of a ‘playboy’. Nevertheless, these activities should not detract from the significant contributions he made to advancing heart surgery.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
