
Case Report | DOI: https://doi.org/10.31579/2641-0419/420
Department of Cardiac Anaesthesia, Institute of Critical Care and Anaesthesiology, Medanta-The Medicity, Gurugram (Haryana)-122001, India
*Corresponding Author: Ajmer Singh, Department of Cardiac AnaesthesiaInstitute of Critical Care and AnaesthesiologyMedanta-The Medicity, Gurugram (Haryana)-122001, India.
Citation: Ajmer Singh, Ravina Mukati, (2024), Chordal Entanglement following MitraClipTM Implantation Necessitating Open Heart Surgery, J Clinical Cardiology and Cardiovascular Interventions, 7(12); DOI: 10.31579/2641-0419/420
Copyright: © 2024, Ajmer Singh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 September 2024 | Accepted: 30 October 2024 | Published: 29 October 2024
Keywords: transcatheter intervention; Mitraclip implantation; chordal entanglement; open heart surgery
MitraClip implantation has become an alternative technique to reduce the severity of mitral regurgitation for patients with prohibitive surgical risk. It can, however, lead to either procedure-related or device-related complications. Here, we describe a patient which the MitraClipTM arms were entangled to the chordae tendinae and papillary muscles, and the device could neither be deployed nor removed. The patient required open heart surgery for the removal of the clips and emergent MV replacement. The remaining perioperative course and follow-up of the patient was unremarkable.
For the last two decades, mitral valve (MV) edge-to-edge repair by MitraClipimplantation has become the most popular, alternative technique to alter the mitral valve morphology, annular diameter, and reduce the severity of mitral regurgitation (MR) for patientswith prohibitive surgical risk.1 Since the first MitraClip implantation in 2003, over 200,000 patients have undergone this procedure worldwide.2 The MitraClip implantation is a transcatheter method that is similar to the Alfieri technique in that it connects the middle scallops of the anterior (A2) and the posterior (P2) leaflet of a regurgitant MV. Echocardiography is an essential imaging modality for patient selection, guidance of the procedure, the identification of periprocedural complication/s, and the evaluation of the final result after clip implantation. The MitraClip implantation can cause procedure-related or device-related complications.3 The procedure-related complications include cardiac perforation, cardiac tamponade, vasculartrauma/dissection, cardiac arrhythmias, myocardial infarction, stroke, bleeding, thrombosis, and infective endocarditis. The device-related complications include leaflet perforation, leaflet tear, dislodgement of the device, single leaflet device attachment, and chordal entanglement/ entrapment/rupture. We report a case in which the MitraClipTM arms were entangledto the chordae tendinae and papillary muscles,and the device could neitherbe deployed nor removed. The patient required open heart surgery for the removal of the clips andemergent MV replacement.
A 72-year-old man was admitted to our institution for worsening dyspnea (New York Heart Association functional class III) for the last two months. Clinical evaluation and investigations including echocardiography revealed degenerative MV disease causing severe MR. The specific signs of severe MR included a vena contracta width of 0.8 cm, a large central regurgitant jet occupying >40% of the left atrium, systolic flow reversal in the pulmonary veins, a dense continuous-wave Doppler MR jet with a peak velocity of 5.1 cm/s, effective regurgitant orifice area of > 0.4 cm2 (Figure 1), dilated left atrium (5.7 cm), and enlarged left ventricle (end- diastolic dimension 6.0 cm). The MV leaflets were thickened with prolapse of the anterior mitral leaflet and tethered posterior leaflet (Figure 2). The left ventricular ejection fraction (LVEF) was 30%. The co-morbid conditions included systemic hypertension, type II diabetes mellitus, chronic obstructive pulmonary disease, and chronic kidney disease (serum creatinine 2.7 mg/dl). The calculated EuroSCORE II for MV repair/replacement was 7.2%. Given the symptoms, echocardiography findings, and co-morbid conditions, the ‘Heart-team’ advised percutaneous MitraClipTM edge-to-edge repair and informed consent was obtained.
Under standard cardiac monitoring including three-dimensional transesophageal echocardiography (TEE, X7-2t probe, Philips), general anesthesia was induced in the hybrid operating room. The cardiac surgical team and cardiopulmonary bypass (CPB) machine were kept on standby. Using fluoroscopy and TEE guidance, the MitraClipTM G4 XTW (Abbott Laboratories, Abbott Park, IL, USA) implantation procedure was started.
The standard procedural guidelines were followed which included trans- septal puncture in the superior and posterior part of the interatrial septum (Figure 3), introduction of the steerable guide catheter and clip delivery system into the left atrium, positioning of the MitraClipTM perpendicular to the MV plane and coaptation line of MV leaflets, and advancing it into the left ventricle (Figure 4). After grasping the leaflets (A2 and P2) between the clip arms and the grippers, the clip was closed, but there was a residual lateral jet causing 3+ MR (Figure 5). The second clip was deployed as parallel as possible and lateral to the first one, but still, there
was 3+ MR. We attempted to implant a third device but grasping was suboptimal and an entrapment of the device in the subvalvular apparatus was suspected on TEE. All possible maneuvers to release the device failed, and the decision to remove it by open heart surgery was taken. During surgery, the MitraClipTM arms entangled with chordae and papillary muscles were removed (Figure 6) and the MV was replaced by using a 25 mm SJM Epic mitral tissue valve. Follow-up visits at three and six months showed normal functioning of the bioprosthetic MV.
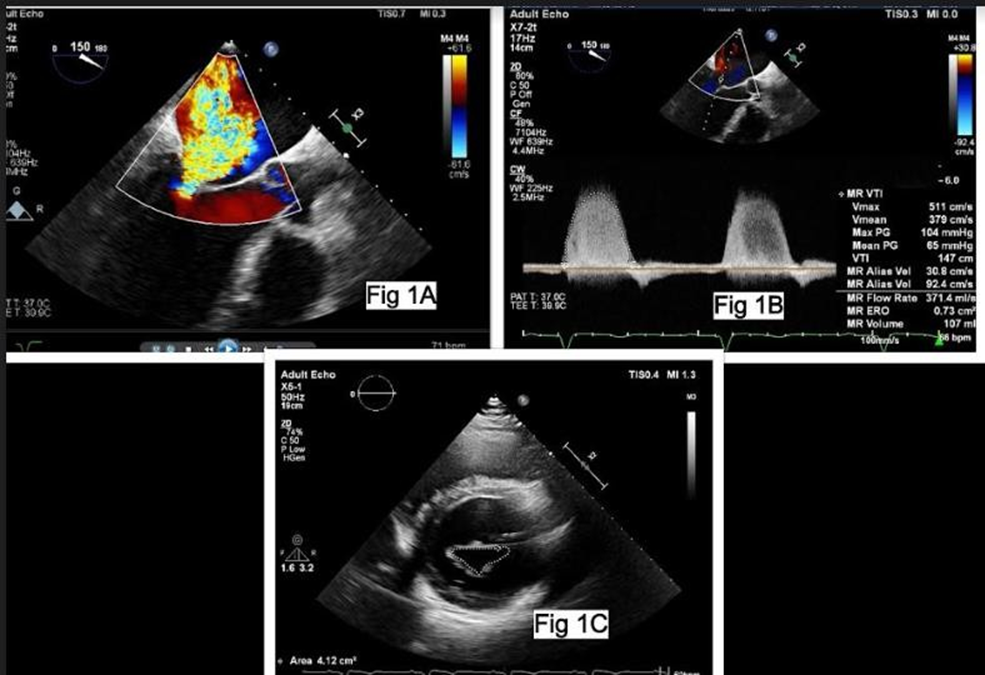
Figure 2: Three-dimensional en-face view of the mitral valve showing prolapse of the anterior mitral leaflet (white arrow), tethered posterior leaflet (black arrow, Figure 2A), and a central jet of severe mitral regurgitation (Figure 2B)
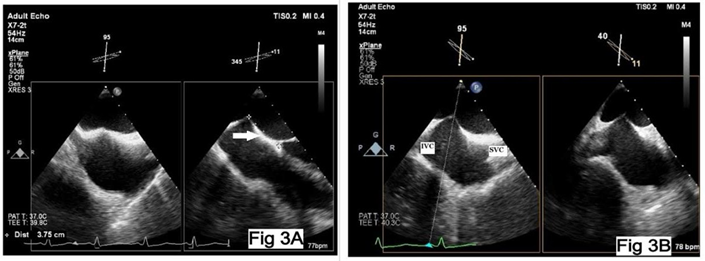
Figure 3: X-plane view of the interatrial septum depicting the site of trans-septal puncture (Fig 3A) at thesuperior and posterior part (Figure3B). SVC: superior vena cava, IVC: inferiorvena cava
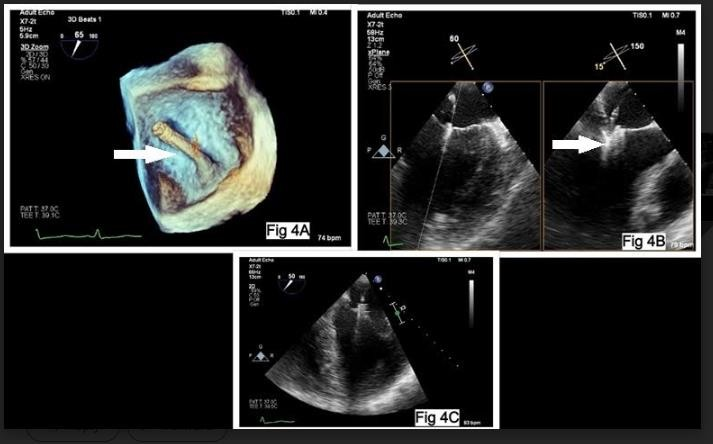
Figure 4: Introduction of the steerable guide catheter (arrow, Figure 4A) and clip delivery system into the left atrium (Fig 4B), and positioning of the MitraClipTM into the left ventricle (Figure 4C)
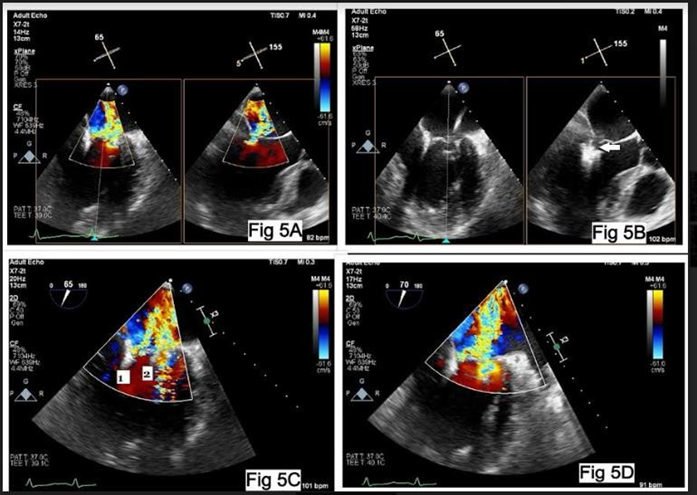
Figure 5: Residual mitral regurgitation after implantation of first clip (Figure 5A) due to non-coaptation of leaflets (arrow, Figure 5B). Residual mitral regurgitation after implantation of clip 1 and 2(Fig 5C) and final result showing severe mitral regurgitation (Figure5D)
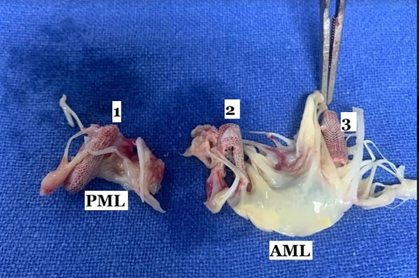
Figure 6: MitraClipTM arms (1, 2, and 3) entangled with chordae of the posterior mitral leaflet (PML) and anterior mitralleaflet (AML) removedduring surgery
The most plausible explanation for the entrapment of chordae and papillary muscles in this patient is the inappropriate positioning of the MitraClipTM. There is also a possibility that the clip might have rotatedduring translation from the left atrium to the left ventricle. The first step to extract the entangled clip includes the reversal of the most recent maneuversto the MitraClipTM. On the contrary,a considerable adjustment in clip arm orientation in the left ventricle can itself result in clip- entanglement in the subvalvular apparatus. If the clip position is not satisfactory, raising the grippers and inverting the clip-arms, followed by retracting the inverted clip-arms into the left atrium may be helpful. Entanglement of the devicein the subvalvular apparatus prevented raising the grippers and inverting the clip-arms in this patient. If the clip cannot be removed despite exhaustive attempts, an option is to deploy the clip onto the entangled subchordal mitral apparatus and remove it surgically, ratherthan tearing chords.The MitraClipTM procedureis preferably performedin the hybrid operating room, a location capable of handling CPB and open-heart surgery.4 The advantages of a hybrid room includethe immediate availability of critical personneland resources, such as additional anesthesiologsts, perfusionists, and CPB equipment. Severely impaired LVEF and comorbidities make MitraClipTM candidates less suitable for surgery. Franzen et al5 demonstrated that MitraClipTM implantation can be safely performed with promising results in patients with very reduced LVEF as 34% of their patients had an LVEF <20>
In a recent study performed by Chhatriwalla et al, the complication rate of MitraClipTM implantation was 8.5%.6 They assessed the relationship between operator experience and procedural results of the MitraClipTM in a cohort of 14,923patients and found that 1,266 developed complications related to the procedure. The complications that arose due to the clip implantation itself, included: single leaflet device attachment partial clip detachment, isolated leaflet damage,clip embolization, conversion to open heart surgery, and lack of procedural success. Mid- term results of the EVEREST trial have reported a conversion rate of 1.8% for open heart surgery and a procedural failure rate of 26%.7 With the development of technology and the availability of ‘extended clip- arms’ the risk of partial clip detachment has reduced from 11% to 0.2%. Another complication that requires urgent conversion to open heart surgery is clip embolization. Fortunately, it is extremely rare and constitutes only 0.1% of the cases.3An anatomic variant,the intermediate accessory papillary muscle, and central chordae tendineae originating from it can impede the smooth handling of the clip and increase the risk of clip entanglement during the procedure.8
Compared to other transcatheter therapies such as transcatheter aortic valve implantation, periprocedural complication rates of MitraClipTM implantation are relatively low. Nevertheless, complications such as entanglement of the device in the subvalvular apparatus necessitating open heart surgery can happen.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
