
Opinion | DOI: https://doi.org/10.31579/2639-4162/109
Specialist in Family and Community Medicine Health Center Santa Maria de Benquerencia. Regional Health Service of Castilla la Mancha (SESCAM), Toledo, Spain.
*Corresponding Author: Jose Luis Turabian, Health Center Santa Maria de Benquerencia. Regional Health Service of Castilla la Mancha (SESCAM), Toledo, Spain.
Citation: Jose Luis Turabian, (2023), Child Care Versus Adult Care the two sides of the same Coin: Familiar Care, J. General Medicine and Clinical Practice. 6(6); DOI:10.31579/2639-4162/109
Copyright: © 2023, Jose Luis Turabian. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 13 March 2023 | Accepted: 21 April 2023 | Published: 10 November 2023
Keywords: family systems; family characteristics; childhood family factors
In many places, medical care for children and adults is carried out by different professionals: paediatricians and general practitioners (GPs). Although this division, like others in medicine, is based on logical reasons of specialization in certain tasks, it entails significant risks, if the pediatrician or GP attends to the child or adult without taking into account that they are inserted in a family system
In many places, medical care for children and adults is carried out by different professionals: paediatricians and general practitioners (GPs). Although this division, like others in medicine, is based on logical reasons of specialization in certain tasks, it entails significant risks, if the pediatrician or GP attends to the child or adult without taking into account that they are inserted in a family system, and not understanding that the explicit reason for consultation, very often, hides a latent reason of the family. Thus, for example, the child who is repeatedly taken by his mother to the pediatrician for upper respiratory infections or infections that "do not heal", and who is treated as such repeatedly by the pediatrician, may mean a request for help from the mother instead of a child's illness. It can be said that an important characteristic of pediatrics and general medicine is to take into account family members in the care of individual patients, although in real life the family approach is variable (1, 2). In addition, the different styles used by physicians to focus on the family affect the process and outcomes of care for the patient (child or adult) (3, 4). Thus, there are some basic concepts of contextualized care in the family that both pediatricians and GPs should take into account, they are: 1.-The family is the primary source of beliefs and behaviors about health; 2.-The stress that the family feels when going through developmental transitions can manifest as physical symptoms; 3.-Somatic symptoms may have an adaptive function within the family and be maintained by family patterns; and 4.-Families are important sources of resources and support for managing the disease. Families play an essential role in people's health and illness (5). A wide range of diseases show some degree of clustering in families (6). The family structure influences the patterns of use of medical services, the reasons for consultation and therapeutic compliance of children and adolescents (7, 8). Family support affects the outcomes of numerous health problems. The disease usually occurs at times of crisis or transitions in the family (9). Families transmit some diseases directly through the biological transfer of DNA. Many diseases have significant genetic factors that increase the likelihood of developing them, including depression, alcoholism, breast cancer, colon cancer, and the onset of diabetes mellitus in adult life, although genetic risks can be reduced or increased by long-standing behavioral patterns that have their origin in the family unit (10). Even when the patient apparently appears alone in the visit, with him/her virtually enters all his network of relationships in his context and beliefs; and the person's main network of relationships is the family. Doctor-patient relationship is actually triangular: doctor-patient-family. The doctor is in contact with the patient for a few minutes, but the rest of the time he is in contact with his family. Therefore, the family must be considered as a fundamental element for treatment (hygienic measures, diets, risk of obesity, taking drugs, exercise or rest, risk behaviors, including substance use, smoking and drinking, etc.) (11 -14). Families play an essential role in people's health and illness, to the point that family support can affect the health outcomes of the individual, and sometimes the illness arises in times of family crisis (15). Thus, for example, compared to young people from well-functioning nuclear families, young people from discordant nuclear families show worse physical and mental health, their parental fixation is not as strong, they tend to drink more alcohol, smoke more cigarettes and use more soft drugs (16). An individual's problems are usually best understood when placed in the context of the family. Problems are often shared by more than one individual in the family. The family itself may hold the key to successful solutions. Any disease has an impact on the other members of the family. There are situations in which family members may be contributing to an individual's symptoms or health problems. There are circumstances in which illness in one family member correlates with increased or decreased symptoms in another member. The family affects the health of its members and is affected by them. Thus, the family can, 1) be the cause of illness due to a health problem, low income, low educational level, poor family relationships, altered family functioning, negative life events, etc. These factors may be associated with schizophrenia, depression, psychosomatic illnesses, infections, alcohol abuse, anorexia nervosa, etc., in other family members (17-20); And 2) There are effects of illness in the family: chronic illness and disability, acute illness, caregivers, sick children, loss of family members (fear of loss or real loss) (21-23). The degree of doctor-patient cooperation is related to the degree of doctor-family cooperation. The more complex the problem to be addressed the greater the need to work with the family group. Pediatrician or GP who does not look at the patient's family is not being aware of a basic law of Nature: the "billiard ball" effect, that is, that the family affects the health of its members and is affected by them. And if we work with a contextualized approach in the patient's family (child or adult), what do we need to know about the family in terms of health? Well, it depends on the use we plan to make with that information. And how can we organize the almost limitless data that can be collected from families? Basically we need to find "the system that defines the problem" (24): the set of people affected by the problem, both in terms of maintenance and treatment. In summary, the pediatrician and the GP should be attentive to certain signs that indicate the need for family evaluation (TABLE 1) (25-27).
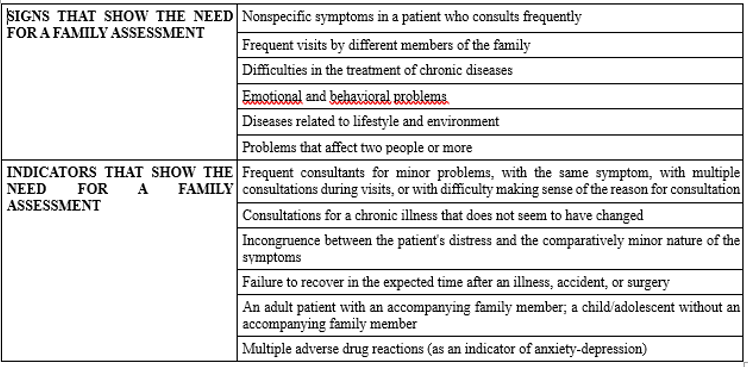
Table 1: Signs and Indicators That Show the Need For Family Assessment
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
