
Research Article | DOI: https://doi.org/10.31579/2690-4861/676
1Graduate Program in Speech-Language Pathology, Department of Speech-Language Pathology, Federal University of Rio Grande do Norte, Natal, Rio Grande do Norte, Brazil.
2Multiprofessional Preceptor Neuropsychologist, Santos Dumont Institute, Macaíba, Rio Grande do Norte, Brazil.
3Multiprofessional Preceptor Speech-Language Pathologist, Santos Dumont Institute, Macaíba, Rio Grande do Norte, Brazil.
4Department of Speech-Language Pathology, School of Dentistry, University of São Paulo, São Paulo, Brazil.
*Corresponding Author: Fernanda Vanessa da Costa Varela, Graduate Program in Speech-Language Pathology, Department of Speech-Language Pathology, Federal University of Rio Grande do Norte, Natal, Rio Grande do Norte, Brazil.
Citation: Fernanda Vanessa Da Costa Varela, Sarah Camilla Ferreira De Oliveira Lima, Mirelly Danglês de Oliveira Ferreira, Dionísia Aparecida Cusin Lamônica, Cíntia Alves Salgado Azoni, (2025), Characterization of Written Language Skills in Children and Adolescents with Myelomeningocele, International Journal of Clinical Case Reports and Reviews, 25(1); DOI:10.31579/2690-4861/676
Copyright: © 2025, Fernanda Vanessa da Costa Varela. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 March 2025 | Accepted: 28 March 2025 | Published: 09 April 2025
Keywords: meningomyelocele; reading; educational status; learning
Myelomeningocele (MMC) is a type of open spina bifida caused by the improper closure of the neural tube during development, which can lead to motor, neurological, and cognitive impairments. Recurrent hospitalizations may negatively impact development and literacy acquisition. Understanding this population's reading and writing challenges is essential for transforming their educational practices. This study aimed to characterize the written language skills of children and adolescents with MMC. This cross-sectional, quantitative, qualitative study involved nine children and adolescents with MMC of both sexes, aged 7 to 15 years, with academic difficulties. They were assessed regarding intellectual capacity, phonological awareness, rapid automatized naming, phonological working memory, reading and writing words and nonwords, identifying graphical aspects of writing, and attitudes toward reading. The results showed that all participants performed worse in the execution than the verbal domain; six performed below expectations in phonological awareness, with the greatest deficits at the phoneme level; four had impairments in rapid automatized naming; six performed below expectations in phonological working memory, with severe deficits in reading and writing. Moreover, four participants had graphic changes consistent with signs of dysgraphia. Despite these challenges, all participants were interested in reading and writing. It is concluded that the children and adolescents in this study had difficulties in skills related to reading and writing development but were interested in and enthusiastic about reading.
Myelomeningocele (MMC) is a type of spina bifida caused by the improper closure of the neural tube during the gestational period. It is characterized by an alteration in the spinal cord located at any point along the spine, marked by the presence of a skin-covered sac with nerves, cerebrospinal fluid, and the spinal cord (Melo et al., 2018; Matson et al., 2005).
Moreover, Arnold Chiari type II malformation, hydrocephalus, motor impairments, neurogenic bladder and bowel, intellectual disabilities, and emotional, social, and psychosocial disorders may be comorbid with this condition (Fletcher et al., 2020). External ventricular drain (EVD) procedures are used to drain cerebrospinal fluid and manage hydrocephalus, a condition present in almost all cases of MMC. However, this technique may fail throughout the person's development, leading to recurrent hydrocephalus symptoms and, consequently, the need for additional drain replacement surgeries (Takoutsing et al., 2023).
Folic acid deficiency is among the various causal factors of MMC (one of the most common malformations among live newborns) and a significant risk factor for improper neural tube development. Other factors, such as the family's socioeconomic status, may also be related to the causes of MMC (Silva et al., 2018; Au et al., 2010).
MMC is classified into functional levels based on the analysis of its neurological involvement, which can be thoracic, lumbar, or sacral (Argento et al., 2011). This functional classification is linked to daily life activities and facilitates care throughout the individual's lifespan (Rethlefsen et al., 2021).
The neuropsychological phenotype of MMC may vary qualitatively, especially when associated conditions such as hydrocephalus are present. Nevertheless, it is often linked to central deficits in processing speed, attention, and movement that emerge early in development (Wasserman et al., 2016).
This population faces difficulties in word decoding and reading comprehension during their reading and writing development, which enhanced by personal factors, lead to academic challenges and a slower literacy acquisition (Pike et al., 2013; Yates, 2003). Furthermore, challenges in integrating these children into the school environment help delay their literacy process (Pike et al., 2013; Salomão et al., 1995).
In addition to health-related challenges, children and adolescents with MMC who attend school may lack accessibility in these environments (Freitas et al., 2020). They may also encounter other daily barriers, which can negatively impact their development (Pike et al., 2013; Salomão et al., 1995).
Reading and writing are essential for inclusion, social participation, access to information, and professional development. Studies on the relationship between individuals with MMC and written language are increasing (Pike et al., 2013; Lamônica et al., 2011; Rozensztrauch, Iwanska & Baglaj, 2021). Therefore, understanding the functioning of individuals with MMC regarding written language development is of utmost importance.
Considering these people’s neurological and social aspects, this study hypothesized that children and adolescents with MMC may have impaired written language performance, given the multidimensional nature of the condition. Thus, the study aimed to characterize written language skills (phonological processing, reading, and writing) and intellectual skills of children and adolescents with MMC.
This cross-sectional, quantitative, qualitative study characterized the written language skills of children and adolescents with MMC, participants of the Pediatric Spinal Cord Injury Clinic at a Brazilian Specialized Rehabilitation Center. It was approved by the Research Ethics Committee under evaluation report no. 5.132.945.
This Pediatric Spinal Cord Injury Clinic serves 27 children and adolescents undergoing physical, occupational, and speech-language-hearing therapy, nutritional, psychological, and medical treatment, and social assistance. Participants were selected based on the inclusion criteria: age (7 to 15 years), both sexes, diagnosis of MMC, with reading and writing difficulties reported by the caregivers, the participants, and/or the therapists who worked with them, and an intellectual level appropriate for their chronological age according to neuropsychological assessment. The exclusion criteria were other associated diagnoses. All participants underwent prior audiological and neuropsychological evaluations. All participants had hearing results within normal limits. In the neuropsychological evaluation, participants who did not have an average IQ were excluded. By applying these criteria, nine children and adolescents aged 7 to 15 years were selected by convenience (since they were treated at the clinic). The other participants did not meet the criteria due to inability to attend study sessions regularly, age outside the 7-15-year range, or lack of written language issues.
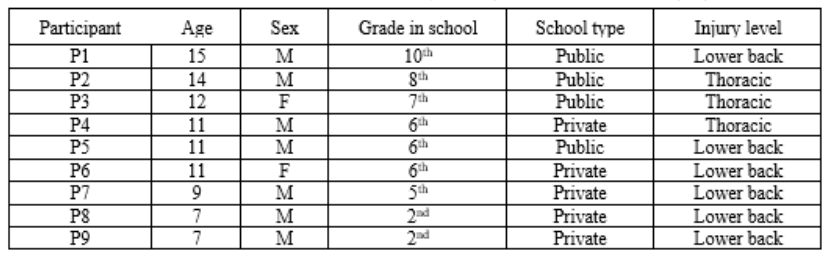
Table 1: Characterization of the sample.
Characterization of the sample:
All nine (100%) participants underwent surgery to correct MMC within the first 24 hours of birth. All had hydrocephalus and had a drain inserted – a fundamental procedure for relieving intracranial pressure. Moreover, all participants had drain corrections throughout their development, requiring recurrent hospitalizations, and hindering their development.
Chart 1. Number of external ventricular drain revisions per participant.
Regarding birth and development data in the first years of life, one participant (P9) was premature (35 weeks) and had jaundice, requiring 12
days in the ICU to adjust bilirubin levels. This same participant had a tethered spinal cord throughout development and underwent surgical procedures to correct the issue. Two participants (P3 and P9) experienced seizures when younger and took phenobarbital for less than 2 years after the seizures. One participant (P8) was diagnosed with Chiari Type 2 syndrome and strabismus. All participants have been enrolled in multidisciplinary therapies since the first year of life, including psychological, physical, occupational, and speech-language-hearing therapy (focused on dysphagia and oral language). Only two of the nine participants do not use a wheelchair.
The sample comprised nine participants – seven (78%) males and two (22%) females. Five (56%) attended private schools, and four (44%) attended public schools. Moreover, six (67%) participants had a lower-back injury, and three (33%) had a thoracic injury.
The participants and their families were informed about this study and signed informed assent and consent forms, respectively.
The participants’ parents/guardians initially answered a semi-structured medical history survey, providing prenatal, perinatal, and postnatal information. They reported on surgeries to correct MMC and hydrocephalus, the need for subsequent surgeries, neuropsychomotor development, and the participant's literacy process. Next, their written language was assessed. The study used the following instruments:
Neuropsychological assessment:
a) Intellectual Capacity Screening: The Wechsler Abbreviated Scale of Intelligence (WASI) is an intelligence assessment instrument applicable to individuals aged 6 to 89 years (Wechsler et al., 2014). It provides a brief and psychometrically reliable measure of intelligence (Yates et al., 2006), providing information on total intelligence quotient (TIQ), performance IQ (PIQ), and verbal IQ (VIQ) through the application of four subtests (Vocabulary, Block Design, Similarities, and Matrix Reasoning). These subtests evaluate various skills, including fluid and crystallized intelligence, verbal knowledge, visual processing, and visuospatial reasoning (Malloy-Diniz et al., 2016). As a psychological test, the WASI is exclusively for use by psychologists, as stipulated in Paragraph 1 of Article 13 of Brazilian Law no. 4.119/62. Therefore, its content cannot be included in the Annex. Accordingly, this research had the WASI administered by psychologists registered with the Regional Council of Psychology of Rio Grande do Norte, Brazil (CRP-17).
Speech-language-hearing assessment:
a) Evaluation of Phonological Awareness, using the Sequential Assessment Instrument (CONFIAS) (Moojen et al., 2003). This test assesses phonological awareness – i.e., the ability to reflect on and manipulate speech sounds comprehensively and sequentially. This allows for the investigation of phonological skills in relation to spelling hypotheses.
b) Automatized Naming Assessment using the TENA Automatized Naming Test) (Silva, Mecca, & Macedo, 2018), which estimates the person's ability to recognize a visual symbol and name it accurately and quickly.
c) Phonological Working Memory Assessment using the Nonword Repetition Test (Grivol & Hage, 2011), which assesses the memory responsible for storing information temporarily to support performance in various cognitive tasks. It consists of nonwords with low, medium, and high similarity and can be used with students starting from the 1st grade.
d) Reading and Writing Assessment using the School Performance Test (TDE II) (Stein, 1994), which objectively assesses fundamental academic performance skills, specifically in writing, arithmetic, and reading. It provides a comprehensive overview of which areas of academic learning are preserved or impaired in the examinee. This study did not include the arithmetic test.
e) Dictated Text Writing, using the Dysgraphia Scale proposed by Lorenzini (1993). Participants are provided with a sheet of paper and a no. 2 black pencil. The scale allows for a quantitative analysis of writing based on scores assigned to 10 analysis items.
f) Scale of Attitudes Toward Reading (Condemarim & Medina, 2005), consisting of a sheet with a character depicted in four poses (very happy, content, annoyed, and very bored/uneasy). The child is asked to respond to seven reading-related questions and mark with an "X" the corresponding profile.
The results of the medical history survey, intellectual capacity screening, phonological awareness assessment, rapid automatized naming, phonological working memory, reading, and writing were analyzed qualitatively and descriptively, in accordance with the expected outcomes. The Shapiro-Wilk normality test was used regarding the sample distribution, indicating a non-normal distribution of the research participants. The results are presented in tables.
All caregivers reported the participants had difficulties with reading and writing skills and the literacy process.
The study found a significant difference (p = 0.05) in the participants’ performance in VIQ (assessing expressive language, oral skills, verbal reasoning, and concept formation and summarization), PIQ (assessing non-verbal concept formation, visual perception and organization, simultaneous processing, and visuomotor coordination), and TIQ (Wechsler et al., 2014). VIQ was higher (M = 109.7; SD = 18.9) than PIQ (M = 85.9; SD = 14.1), when compared to the normative data expected for their age (Table 2).
| Participant | IQ | Verbal Classification (VIQ) | IQ | Performance Classification (PIQ) |
| P1 | 97 | Average | 63 | Much lower |
| P2 | 93 | Average | 92 | Average |
| P3 | 69 | Extremely low | 66 | Extremely low |
| P4 | 131 | Much higher | 104 | Average |
| P5 | 102 | Average | 72 | Threshold |
| P6 | 106 | Average | 75 | Threshold |
| P7 | 131 | Much higher | 97 | Average |
| P8 | 132 | Much higher | 95 | Average |
| P9 | 129 | Superior | 103 | Average |
Caption: IQ = intelligence quotient
Table 2: Classification of the verbal and performance domains (Condemarim & Medina, 2005).
Moreover, they performed significantly lower in PIQ than the normative average (t = -3.59, p = .005). No significant differences were found in TIQ between the participants (M = 96.9 σ = 17.4).
Regarding the reading predictors involving phonological processing, three participants (P2, P4, and P7) performed as expected in phonological
awareness at both the syllable and phoneme levels according to the alphabetic spelling hypothesis, while the others (n = 6, P1, P3, P5, P6, P8, and P9) had results consistent with the syllabic-alphabetic spelling hypothesis. These results align with these children’s writing level in the written assessment. All participants had greater difficulty in the phoneme level than in the syllable level (Table 3).
| Participant | Syllabic level | Spelling hypothesis | Phoneme level | Spelling hypothesis | Total performance |
| P1 | 33 | Syllabic-Alphabetic | 12 | Syllabic-Alphabetic | 45 |
| P2 | 40 | Alphabetic | 24 | Alphabetic | 64 |
| P3 | 26 | Syllabic-Alphabetic | 17 | Syllabic-Alphabetic | 43 |
| P4 | 39 | Alphabetic | 26 | Alphabetic | 65 |
| P5 | 31 | Syllabic-Alphabetic | 14 | Syllabic-Alphabetic | 45 |
| P6 | 26 | Syllabic-Alphabetic | 17 | Syllabic-Alphabetic | 51 |
| P7 | 37 | Alphabetic | 29 | Alphabetic | 66 |
| P8 | 35 | Alphabetic | 12 | Syllabic-Alphabetic | 47 |
| P9 | 25 | Syllabic-Alphabetic | 17 | Syllabic-Alphabetic | 42 |
Caption: All participants were expected to be in the alphabetic spelling hypothesis.
Table 3: Participants' performance in the phonological awareness assessment according to the spelling hypothesis (Ferreiro & Teberosky, 1991).
Moreover, only three children performed according to the reference standards in automatized naming (Silva, Mecca, & Macedo, 2018). The percentiles and results show that P7’s and P8’s results were average in colors, letters, and objects and below average in digits. P9’s performance was below average in colors, letters, and digits and inferior in objects. The other participants (n = 6) did not have their values compared to their ages, as the reference standards provided comparative data for children aged 3 years to 9 years and 11 months (Silva, Mecca, & Macedo, 2018). Thus, a qualitative analysis comparing the group's performance with the instrument’s maximum reference showed that only P2 and P4 had results above average in all stimuli, whereas the others (n = 4) had inferior results in letters and digits and average, below average, and inferior results in the other fields (Table 4).
| Part | C (s) | Perf | Perc | L (s) | Perf | Perc | D (s) | Perf | Perc | O (s) | Perf | Perc |
| P1* | 51 | A | 50 | 47 | I | 10 | 49 | I | 10 | 52 | BA | 25 |
| P2* | 33 | AA | 90 | 18 | AA | 90 | 18 | AA | 90 | 35 | AA | 90 |
| P3* | 69 | I | 10 | 43 | I | 10 | 51 | I | 10 | 45 | A | 50 |
| P4* | 38 | AA | 90 | 20 | AA | 90 | 23 | AA | 90 | 36 | AA | 90 |
| P5* | 58 | BA | 25 | 42 | I | 10 | 54 | I | 10 | 65 | I | 10 |
| P6* | 50 | A | 50 | 33 | BA | 25 | 32 | A | 50 | 49 | A | 50 |
| P7 | 46 | A | 50 | 30 | A | 50 | 39 | BA | 25 | 46 | A | 50 |
| P8 | 56 | A | 50 | 40 | A | 50 | 53 | BA | 25 | 45 | A | 75 |
| P9 | 60 | BA | 25 | 44 | BA | 25 | 53 | BA | 25 | 77 | I | 10 |
Caption: Part = participant; C = color; Perf = performance; Perc = percentile; L = letters; D = digits; O = objects; s = time in seconds; A = average; I = inferior; AA = above average; BA = below average; * = patients whose ages were above the protocol’s reference standards.
Table 4: Participants' automatized naming performance (Silva, Mecca, and Macedo, 2018).
Only two children performed according to the reference standards in phonological working memory (Grivol & Hage, 2011). P8 performed as expected only in nonword repetition, while P9 achieved the expected value only in backward digit repetition. All other participants (n = 7) completed the activities in full. The comparison of their results (they were above 9 years old) with the test’s reference standards (8 years and 11 months) showed that all scored more than 69 points in nonword repetition, but only P2 reached the reference value in forward and backward digit repetition. The others (n = 6) had results below expectations in different parts of the protocol – nonword, forward, or backward digit repetition (Table 5).
| P | CR | ECR | T (s) | ET (s) | CW | ECW | T (s) | TE (s) |
| P1* | 5 | 30 | I | 60 | 0 | 21 | I | 336 |
| P2 | 32 | 30 | 52 | 60 | 12 | 21 | 302 | 336 |
| P3 | 5 | 29 | I | 77 | 1 | 14 | I | 355 |
| P4 | 29 | 28 | 82 | 89 | 12 | 12 | 389 | 424 |
| P5 | 27 | 28 | 87 | 89 | 4 | 12 | I | 424 |
| P6 | 23 | 28 | 96 | 89 | 0 | 12 | 526 | 424 |
| P7 | 32 | 28 | 91 | 97 | 19 | 8 | 336 | 410 |
| P8 | 27 | 23 | 142 | 155 | 10 | 14 | 535 | 506 |
| P9 | 26 | 23 | 153 | 155 | 7 | 14 | I | 506 |
Caption: P = Participant; CR = correct reading; ECR = expected correct reading; T = time; s = time in seconds; ET = expected time; CW = correct writing; ECW = expected correct writing; I = interrupted; * = participant whose age was above that of the test
Table 5: Participants’ performance in phonological working memory (Grivol & Hage, 2011).
Regarding reading, the quantitative TDE II analysis showed that P2, P4, P7, P8, and P9 performed as expected for their education level. The others (n = 4) did not reach the minimum expected performance. Moreover, P1, P3, and P6 were unable to read the words within the expected time, and P1 and P3 had to stop the assessment due to difficulties with decoding (Table 6).
| Participant | Reading Classification | Writing Classification |
| P1* | SD | SD |
| P2 | RD | WE |
| P3 | SD | SD |
| P4 | MMD | MMD |
| P5 | SD | SD |
| P6 | SD | SD |
| P7 | AE | AE |
| P8 | SD | SD |
| P9 | SD | SD |
Caption: SD = severe deficit; RD = risk for deficit; WE = within the expected; MMD = mild to moderate deficit; AE = above the expected; * = participant whose education level was above the test’s reference standard.
Table 6: Results obtained in and expected for the TDE II reading and writing subtests (Stein, 1994).
Regarding the writing assessment, P4 and P7 achieved the expected number of correct answers for their education level, with 12 and 19 correct answers, respectively. P2, P4, and P7 completed the subtest within the expected time, whereas four participants (P1, P3, P5, and P9) requested to stop the assessment due to difficulties in word encoding, making it impossible to analyze their testing time. P1's results were compared to those of 9th-graders because their education level was above the one indicated in the protocol (Table 6).
The protocol also interprets the results based on the children’s percentiles and their school types (whether public or private). Only one child (P7) performed above expectations in both reading and writing, whereas P2 performed as expected in reading, and P4 had a mild to moderate deficit. The others (n = 6) had severe deficits in both skills, according to their school types (public or private – Table 7).
| Participant | Reading Classification | Writing Classification |
| P1* | SD | SD |
| P2 | RD | WE |
| P3 | SD | SD |
| P4 | MMD | MMD |
| P5 | SD | SD |
| P6 | SD | SD |
| P7 | AE | AE |
| P8 | SD | SD |
| P9 | SD | SD |
Caption: SD = severe deficit; RD = risk for deficit; WE = within the expected; MMD = mild to moderate deficit; AE = above the expected; * = participant whose education level was above the test’s reference standard.
Table 7: Test interpretation based on percentiles and school types (Stein, 1994).
The text dictation analysis (Lorenzini, 1993) showed that P1, P3, P5, and P9 performed consistently with signs of dysgraphia, as they scored above 8.5 (cursive handwriting) and 6 points (print handwriting). The other participants (n = 5) had inferior results and were not classified with dysgraphia (Table 8).
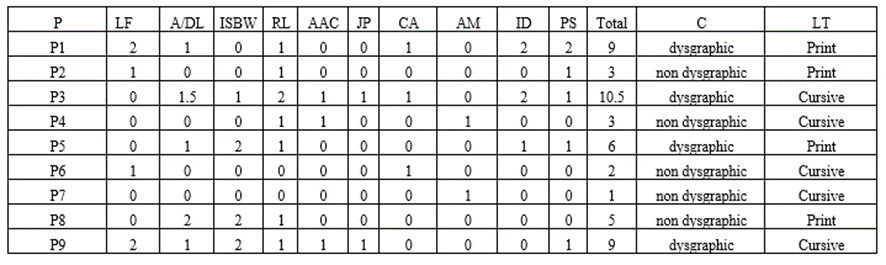
Caption: P = participants; WL = wavering lines; A/DL = ascending/descending lines / ISBW = irregular space between words; RL = rewritten letters; AAC = arch angle curvature; JP = junction point; CA = collisions and adherences; AM = abrupt movements, ID = irregular dimensions; PS = poor shapes; C= classification; LT = letter type
Table 8: Dysgraphia scale results (Lorenzini, 1993).
Although all study participants had intellectual capacity appropriate for their chronological age, the study showed that 67% had difficulties in phonological processing, reading, and writing skills, and had worse results in PIQ than VIQ.
Conditions comorbid with MMC may lead to complications that could interfere with these people’s development, integration into different social environments, psychological-linguistic processes, and learning. The presence of hydrocephalus associated with MMC, the need for surgical drain corrections, and other issues may result in a heterogeneous and complex condition, causing additional impairments that interfere with language development and learning (Mont-Serrat, 2018).
The need for recurrent surgeries and frequent hospitalizations may have influenced the educational process of the children and adolescents in this study, as they interrupt educational activities. This poses another risk factor for literacy delays because they need to be absent from school activities, ultimately slowing them from achieving the expected performance for their age groups and education levels (Cunha, Silva, & Palladino, 2014; Façanha, 2015).
Although the study participants’ intellectual capacity was clearly adequate, the impact on PIQ in MMC’s neuropsychological profile can be explained by this population’s motor difficulties. The latter affect the writing process over their development but do not directly impact their other cognitive skills to acquire reading and writing, especially when considering factors within a broader context (Silva, 2019). Thus, education and health professionals should understand how to assign writing tasks in the classroom or other settings, as these children and adolescents’ time and execution may not be the same as those with typical development.
It is known that phonological processing is essential for proper reading and writing performance (Schoenel et al., 2020). The 67% of children in this study who had phonological awareness difficulties and performed below expectations for their education level (Capovilla & Capovilla, 1998) are still at the syllabic-alphabetic writing stage, although they should already be at the alphabetic stage, according to the spelling hypotheses (Ferreiro & Teberosky, 1991). It is inferred that these children’s literacy difficulties are similar to those of children with learning disorders, who likewise have deficits in phonological awareness and reading and writing performance, although they are different health conditions (Silva & Godoy, 2020; Leite, Alpes, & Mandrá, 2022). Therefore, understanding linguistic and metalinguistic functioning is essential for designing an appropriate intervention regardless of the underlying diagnosis.
The difficulties of the children and adolescents in this study regarding the phoneme level were more pronounced than those at the syllable level, in line with the developmental hypothesis of the hierarchy of learning acquisition. This is because syllables require less analytical thinking than phonemes (Pestun, 2004; Lisboa & Jesus, 2019).
The ability to access the lexicon and process information is also essential for reading and writing development. Rapid automatized naming can provide insights into the speed of lexical access and predict reading speed (Georgiou & Parrila, 2020). Among the 34% of children whose results were compared with the test's reference values, two (P8 and P9) performed below expectations on the overall test, indicating a significant relationship with potential reading difficulties (Georgiou & Parrila, 2020). This is consistent with their below-expected performance in the reading and writing assessments.
Phonological working memory plays a crucial role in the development of written language, as reading requires children to decode letters and convert them into sounds while rapidly memorizing this sequence (Grivol & Hage, 2011). In this sample, the two children whose performances were compared to the test's reference standards showed impairments in repetition skills, whether in nonword or digit repetition. Among the others, a qualitative analysis revealed that 45
Assessment findings and result characterization identified difficulties in phonological processing skills, word and pseudoword reading, writing, spelling, and the PIQ in children and adolescents with MMC. Despite these challenges, the participants were enthusiastic about and interested in reading, which may predict progress and facilitate the written language intervention.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
