
Case Report | DOI: https://doi.org/10.31579/2578-8965/169
Master in Comprehensive Care for Women. Second Degree Specialist Gynecology. Head of the Provincial Group of the Specialty in Havana. Member of the National Specialty Group. Cuba
*Corresponding Author: Georgina Álvarez Medina, Master in Comprehensive Care for Women. Second Degree Specialist Gynecology. Head of the Provincial Group of the Specialty in Havana. Member of the National Specialty Group. Cuba
Citation: Georgina Á. Medina, Taimyr S. Matar, (2023), Characterization of Intrauterine Growth Restriction in Pregnant Women Hospital Gynecology and Obstetrics America Arias Havana, Cuba 2022, J. Obstetrics Gynecology and Reproductive Sciences, 7(3) DOI:10.31579/2578-8965/169
Copyright: © 2023, Georgina Álvarez Medina. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 May 2023 | Accepted: 23 May 2023 | Published: 31 May 2023
Keywords: perceived stress; pregnancy; mental health; psychosocial health; west Shewa; ethiopia
Intrauterine growth restriction (IUGR) is a pathology of multifactorial causes and complex management for the obstetrician. For a fetus, not reaching its growth potential represents a significant increase in the risk of perinatal morbidity and mortality. Cases of IUGR were more frequent in patients between 20 and 34 years of age with associated pathologies such as hypertension (HTN), urinary tract infection (UTI) and preeclampsia. The most frequent route of birth was eutocic births since the caesarean sections performed were mostly by previous caesarean sections. Of a total of 1656 births in 2022, 88 were CIUR, six early and 82 late.
The main objective of this work is to characterize intrauterine growth restriction, for which a descriptive and cross-sectional study was carried out in pregnant women at Hospital America Areas in 2022.

As it is not possible to determine the fetal growth potential for its definition, intrauterine growth tables are used, being accepted as growth normal weight for gestational age between the 10th and 90th percentiles. In addition, clinical elements such as the measurement of uterine height and the estimation of fetal weight are used. The early diagnosis of fetuses with growth disorders is to reduce the morbidity and mortality associated with this problem, using for this purpose at certain times interventions already established.
URGR is indirectly associated with short-term perinatal complications such as: stillbirth, intrapartum asphyxia, hypoglycemia, hypothermia, polycythemia, seizures, coagulopathies, sepsis, hyperbilirubinemia and prematurity [2,3]. These complications result in a significant increase in admissions to intensive care units.
In addition to its relationship with prematurity, those newborns born before 32 weeks of gestation and who have CIUR have higher incidences of complications related to prematurity, requiring ventilatory support for longer periods of time and die in greater numbers than premature infants with adequate for gestational age.
In the long term, it has an adverse impact on child development, presenting alterations in muscle tone, lower IQs than those infants with adequate weight, behavioral disorders and adaptation with repercussions in adult life [4].
In the present study and according to its period of time there were 1656 deliveries, of which 88 were CIUR (6 early and 82 late), there were also 22 small for gestational age.
Table 1 describes the maternal ages of pregnant women where there was CIUR and Table 2 their classification according to the type of CIUR.
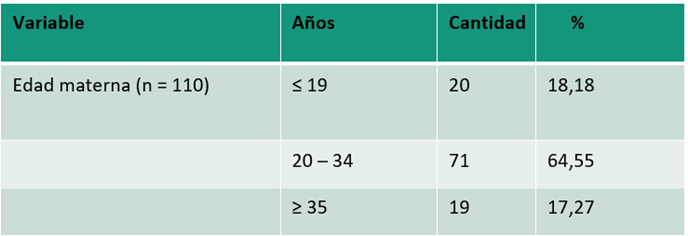
Table 1: Age of pregnant women with CIUR.
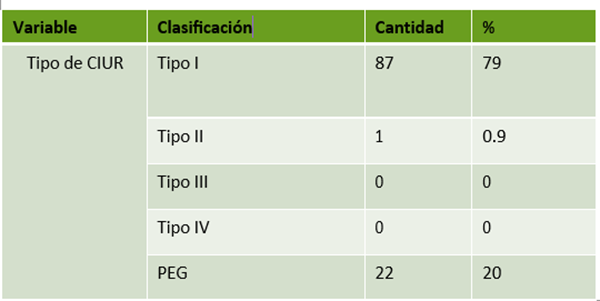
Table 2: Classification of CIUR types.
According to Table 1, the most frequent age were pregnant women between 20 and 34 years for 64.55%, with ages less than or equal to 19 there were 20 pregnant women for 18.18% and with 35 and more years 19 pregnant women for 17.27%.
According to Table 2, the predominant type of URIC was type 1 with 79.10%, since these are growth restrictions with hemodynamics normal according to the functions of the Hospital where the study was conducted and no type 3 and 4 CIUR were presented.
Table 3 shows the classification of the CIUR below the third percentile and between the third and tenth. To do this, he relates it to their fetal hemodynamics, finding a high number of CIUR below the third percentile with normal Doppler (31 cases), which suggests genetic causes, infections by TORCH, etc. Another high number is below the third percentile with altered Doppler associated with placental insufficiency in relation to maternal pathologies (22 cases).

Table 3: Patients according to Doppler characteristics and weight.
Table 4 shows that of the group of CIUR studied there was only one early neonatal death and two late fetal deaths related to hypertensive disease, retroplacental hematoma and placental cause.

Table 4: Distribution of perinatal mortality
The following table shows that chronic arterial hypertension, preeclampsia and urinary tract infection were the most frequent pathologies for the presentation of a CIUR.

Table 5: Patients according to associated pathologies
In this study, eutocic delivery predominated, since type 1 URICS had normal hemodynamics. Caesarean sections are mostly related to Previous cesarean section procedures, although it is not the only cause where the indications for risk of loss of well-being and restless fetal status are high (see Table 6).

Table 6: CIUR according to route of delivery and causes
In the study, ICUR type 1 predominated in the results. The CIUR was not a decisive factor in the results of neonatal mortality at Hospital América Arias in the period studied. The most frequent associated pathologies were chronic arterial hypertension, urinary tract infection and preeclampsia. The most frequent route of birth was eutocic births.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
