
Research Article | DOI: https://doi.org/10.31579/2692-9759/193
Department of Cardiology, The Fourth Affiliated Hospital of Soochow University, Suzhou City, Jiangsu Province, P. R. China.
*Corresponding Author: Jinsheng Shen, Department of Cardiology, The Fourth Affiliated Hospital of Soochow University, Suzhou City, Jiangsu Province, P. R. China.
Citation: Hui Xu, Ziyin Huang, Jinsheng Shen, (2026), Characterization of Gut Microbiota in Coronary Heart Disease Combined with Heart Failure with Preserved Ejection Fraction, Cardiology Research and Reports, 8(3); DOI:10.31579/2692-9759/193
Copyright: © 2026, Jinsheng Shen. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 March 2026 | Accepted: 30 March 2026 | Published: 09 April 2026
Keywords: coronary heart disease; heart failure with preserved ejection fraction; gut microbiota; otu; alpha diversity; beta diver
Objective: Gut microbiota imbalance is prevalent in various types of heart failure (HF) patients, and the gut hypothesis of HF is a current research hotspot in the cardiovascular field. However, there is still a lack of research on the characteristics of gut microbiota in patients with heart failure with preserved ejection fraction (HFpEF) caused by coronary heart disease (CHD). Therefore, this study employs high-throughput sequencing to investigate the characteristic changes in gut microbiota in patients with CHD complicated by HFpEF.
Methods: This study enrolled 9 patients diagnosed with HFpEF caused by CHD who attended the Fourth Affiliated Hospital of Soochow University between January 2025 and January 2026, and 16 healthy individuals who underwent health examinations at our hospital. Fecal samples from both groups were analyzed using high-throughput sequencing to compare differences in gut microbiota composition and diversity indices.
Results: In the OTU-based analysis, the rank-abundance curve indicated that the species richness of the gut microbiota in the HFpEF caused by CHD group was lower than that in the healthy control group, but there was no statistical difference in species evenness between the two groups. Statistical analysis of the total number of OTUs revealed that species diversity was also lower in the HFpEF caused by CHD group compared to the healthy control group. Analysis of differences in gut microbiota species composition between the two groups at the genus level showed significant differences in the abundance of five genera: Faecalibacterium (P=0.0198), Dorea (P=0.0126), Abiotrophia (P=0.0414), Mogibacterium (P=0.0243), and Acinetobacter (P=0.0073). Specifically, the abundance of Faecalibacterium was higher in the HFpEF caused by CHD group, while the abundances of Dorea, Abiotrophia, Mogibacterium, and Acinetobacter were lower. Regarding diversity analysis, PCoA based on Beta diversity showed a distinct separation in gut microbiota composition between the two groups (P < 0.05).
Conclusion: The composition of gut microbiota at the genus level differed between the HFpEF caused by CHD group and the healthy control group. Furthermore, both species richness and diversity of the gut microbiota are reduced in the HFpEF caused by CHD group.
Heart failure with preserved ejection fraction (HFpEF) is characterized primarily by diastolic dysfunction and represents the most common type of heart failure (HF) [1]. Coronary heart disease (CHD) is a major cause of HFpEF. However, HFpEF still lacks detailed diagnostic processes and effective treatment strategies, leading to high patient mortality and readmission rates, and often a poor prognosis. The gut hypothesis of heart failure, an emerging concept, provides new insights for the diagnosis and treatment of HFpEF [2, 3].
In our research published in 2022, we found that gut microbiota imbalance was prevalent in HFpEF patients. Compared with healthy individuals, the composition of gut microbiota in HFpEF patients differed at various taxonomic levels, and both species richness and evenness were reduced. However, our previous study targeted all HFpEF patients, whose etiologies varied. Research on the specific characteristics of gut microbiota in HFpEF patients caused specifically by CHD is still lacking [4].
This study utilizes high-throughput sequencing to detect and analyze fecal samples from the HFpEF caused by CHD group and the healthy control group. The aim is to clarify the composition of gut microbiota in patients with HFpEF caused by CHD, thereby facilitating a better understanding of the characteristic changes in gut microbiota during the pathogenesis of this specific patient subgroup and providing new ideas for their future diagnosis and treatment.
Inclusion and Exclusion Criteria
Inclusion criteria for the HFpEF caused by CHD group (Group A): Patients diagnosed with CHD combined with HFpEF at the Fourth Affiliated Hospital of Soochow University between January 2025 and January 2026. HFpEF diagnosis had to conform to the diagnostic criteria in the "Chinese Guidelines for the Diagnosis and Treatment of Heart Failure," and HFpEF must have been clearly caused by CHD [5].
Inclusion criteria for the healthy control group (Group B): Individuals undergoing health examinations at the Fourth Affiliated Hospital of Soochow University. Examination results must have definitively excluded various types of cardiovascular diseases.
Exclusion criteria for both groups: Individuals who had recently used antibiotics or probiotic preparations, those with concurrent intestinal diseases or a history of prior intestinal surgery, and those diagnosed with other diseases known to cause alterations in gut microbiota.
Sample Collection and Sequencing Process
Fecal samples from study subjects were collected and placed in specialized DNA preservation solutions. After collection, DNA was extracted from frozen fecal samples. Primers were then designed according to the requirements of the sequencing platform, and PCR amplification was performed using a two-step method. The amplified products were further purified, eluted, and quantified. Finally, high-throughput sequencing of the processed samples was performed using the Illumina sequencing platform.
Measurement data in this study were analyzed using independent samples t-tests if they followed a normal distribution and had homogeneous variance. If the data showed a non-normal distribution, non-parametric tests were used for inter-group difference testing. PCoA plots were used to visualize the results of Beta diversity analysis.
OTU-Based Analysis
Operational Taxonomic Units (OTUs) are a common classification method in gut microbiota research. This study set a 97% sequence similarity threshold, meaning sequences with ≥97% similarity were clustered into the same OTU. Analysis of the obtained data showed that as the sample size increased, the number of new OTUs gradually decreased, indicating sufficient sample size and credibility of this study. Statistics on the total number of OTUs revealed 470 OTUs in the HFpEF caused by CHD group and 573 OTUs in the control group. Thus, the total OTU count was lower in the HFpEF caused by CHD group compared to the healthy control group, indicating reduced species diversity in HFpEF caused by CHD patients. Based on OTUs, a rank-abundance curve was plotted (figure 1). The shape of the curve indicated that the curve for the HFpEF caused by CHD group was narrower than that of the healthy control group, suggesting lower species richness in the HFpEF caused by CHD group. However, there was no significant difference in species evenness between the two groups.
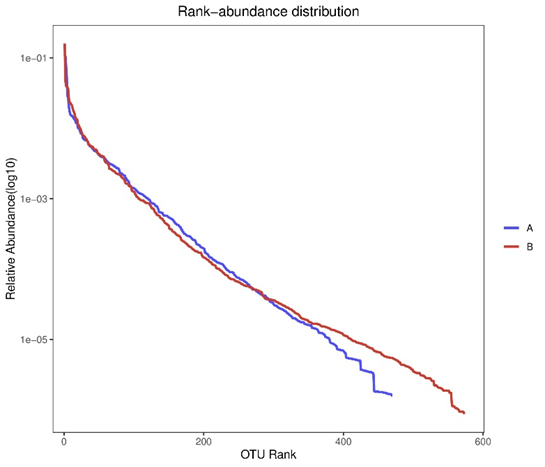
Figure 1: The rank-abundance curve of two groups
Differences in Gut Microbiota Composition Between Groups
According to biological taxonomy, gut microbiota can be classified at seven levels: kingdom, phylum, class, order, family, genus, and species. This study analyzed the composition of gut microbiota samples at the genus level and performed difference tests on the abundance of various species. The results showed that at the genus level, the abundances of five genera differed significantly between the two groups: Faecalibacterium (P=0.0198), Dorea (P=0.0126), Abiotrophia (P=0.0414), Mogibacterium (P=0.0243), and Acinetobacter (P=0.0073). Specifically, the abundance of Faecalibacterium was higher in the HFpEF caused by CHD group compared to the healthy group, while the abundances of the other four genera were lower.
Analysis of Diversity Differences
Diversity analysis is a common statistical method in gut microbiota research. No statistical differences were found in any of the Alpha diversity indices between the two groups in this study. Therefore, Principal Coordinate Analysis (PCoA) based on the Bray-Curtis distance was further performed (figure 2). PCoA plot is a transformation of the data matrix that intuitively and clearly displays the extent of differences between samples. The resulting plot showed a separation trend between the two groups of samples along the PC1 coordinate (P < 0.05).
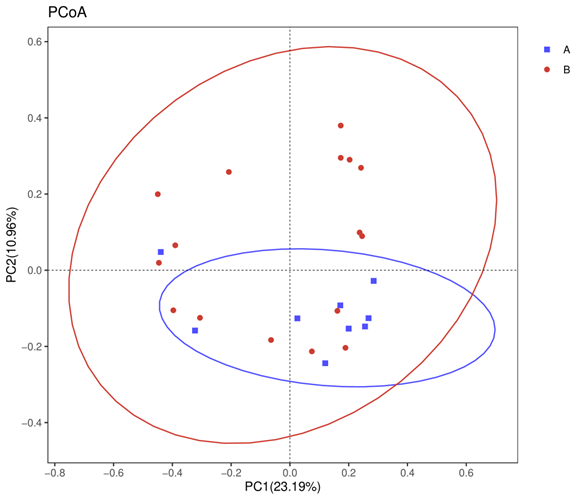
Figure 2: Principal Coordinate Analysis based on the Bray-Curtis distance of two groups.
The gut hypothesis of HF is a current research hotspot in the field of HF, attracting attention from numerous experts domestically and internationally. This hypothesis posits that when HF occurs, the patient's cardiac pump function is significantly impaired, correspondingly reducing intestinal blood flow. Consequently, the intestinal villi and microvilli experience ischemia. Additionally, HF patients often have concurrent intestinal vascular congestion. The combined effect of ischemia and congestion alters the morphology and permeability of the intestinal wall, making gut microbiota prone to translocation and imbalance. This translocation and imbalance can, in turn, influence the progression of heart failure through a series of pathophysiological mechanisms [6,7]. Thus, a close relationship exists between HF and gut microbiota imbalance, and the gut microbiota hypothesis opens a new avenue for the diagnosis and treatment of HF.
According to existing research results domestically and internationally, as well as findings from our team, various types of HF patients exhibit gut microbiota translocation and imbalance. One of the most renowned studies is the report by Luedde et al. on the characteristics of gut microbiota in patients with heart failure with reduced ejection fraction (HFrEF) [8]. By analyzing the gut microbiota of HFrEF patients, they found alterations in its composition and a trend of decreased species diversity [9, 10]. Our team also previously conducted research in this area. By collecting feces from HFpEF patients of various etiologies for high-throughput sequencing and comparing sequencing results across different populations, we found significant gut microbiota imbalance in HFpEF patients, with reduced species richness and evenness compared to healthy controls. However, that study enrolled HFpEF patients with diverse etiologies, and subsequent subgroup analysis revealed differences in gut microbiota among HFpEF patients with different causes [11-13]. Therefore, to further investigate the characteristics of gut microbiota in the specific subgroup of HFpEF patients caused by CHD, we initiated this study.
First, we conducted corresponding data analysis based on OTUs. The rank-abundance graph showed that species richness of the gut microbiota in the HFpEF caused by CHD group was lower than that in the control group, but there was no statistical difference in species evenness between the two groups. Concurrently, we calculated that the total number of OTUs in the HFpEF caused by CHD group was lower than that in the healthy control group, indicating reduced species diversity in the HFpEF caused by CHD group. These preliminary OTU-based analysis results demonstrated differences in gut microbiota between the HFpEF caused by CHD group and the healthy control group.
We further analyzed the composition of gut microbiota between the two groups at the genus level. The results showed that the abundance of Faecalibacterium was higher, while the abundances of Dorea, Abiotrophia, Mogibacterium, and Acinetobacter were lower. Faecalibacterium is a genus of clostridia associated with the production of butyrate and propionate in the body and plays an important role in regulating the immune system [14-15]. The increased abundance of Faecalibacterium in the HFpEF caused by CHD group suggests a potential immune system dysregulation in these patients, which may play a significant role in disease progression. This leads us to hypothesize that Faecalibacterium might serve as a specific marker of gut microbiota alteration in patients with HFpEF caused by CHD, potentially applicable in clinical testing and as a new therapeutic target for this patient group. Currently, methods such as antibiotic use, probiotic administration, and fecal microbiota transplantation are being explored to modulate gut microbiota in experimental animals to treat corresponding diseases. However, research using these approaches to treat HF remains at the animal experimental level, with a considerable journey ahead before clinical application.
In the analysis of Alpha diversity differences between the two groups, none of the indices showed statistical significance. Therefore, we proceeded with PCoA based on the Bray-Curtis distance, and the results further confirmed differences in gut microbiota between the two groups.
In summary, this study clarifies that patients with HFpEF caused by CHD exhibit significant alterations and imbalance in their gut microbiota. This is specifically manifested as reduced richness and diversity of gut microbiota, increased abundance of Faecalibacterium, and decreased abundances of Dorea, Abiotrophia, Mogibacterium, and Acinetobacter in the HFpEF caused by CHD group compared to the healthy group. These alterations in gut microbiota provide new insights for the diagnosis and treatment of patients with HFpEF caused by CHD. However, the sample size of this study is small, and future research with a larger sample size is needed to confirm these findings.
The composition of gut microbiota at the genus level differed between the HFpEF caused by CHD group and the healthy control group. Furthermore, both species richness and diversity of the gut microbiota are reduced in the HFpEF caused by CHD group. The increased abundance of Faecali bacterium in the HFpEF caused by CHD group suggests a potential immune system dysregulation in these patients, which may play a significant role in disease progression. This leads us to hypothesize that Faecalibacterium might serve as a specific marker of gut microbiota alteration in patients with HFpEF caused by CHD.
Funding: This work was supported by grants from Research on Collaborative Innovation of medical engineering combination (SZM2023038), Collaborative Innovation of medical engineering combination (SZM2024036). The funders had no roles in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
