
Research Article | DOI: https://doi.org/10.31579/2692-9562/052
1 Gupta1st Assistant Professor ENT GS Medical College & Hospital Hapur India.
2 Srivastava2nd Consultant ENT, Kingdom of Saudi Arabia (Corresponding author)
32nd Post Graduate Resident ENT PGIMS Rohtak India
*Corresponding Author: Mohit Srivastava, Srivastava2nd Consultant ENT, Kingdom of Saudi Arabia
Citation: Keshav Gupta, Mohit Srivastava, Pratik Kumar (2022). Changing Epidemiology Microbiology and Management Techniques of Retropharyngeal Abscess in Developing Economy in India; Journal of Clinical Otorhinolaryngology 4(3); DOI: 10.31579/2692-9562/052
Copyright: © 2022 Mohit Srivastava. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 April 2022 | Accepted: 22 May 2022 | Published: 25 June 2022
Keywords: retropharyngeal abscess; presentation; diagnosis; management; antibiotic; drainage; practice; current scenario
Aim: Retropharyngeal abscess are potentially fatal infections of deep neck spaces with high morbidity and mortality. We study the current clinical scenario of this fatal infection in the modern world.
Background: Retropharyngeal abscess are considered predominantly as pediatric infections of deep neck spaces. Their prompt diagnosis and management has always presented a challenge to healthcare expert
Study design: This is a retrospective multi-centric study conducted for 3 years at two tertiary care units and comprising 16 cases (2 pediatric and 14 adults). It focuses on each aspect of retropharyngeal abscess in today's world ranging from epidemiology to management to outcome.
Conclusion: We have noted an increase in regional incidence of retropharyngeal abscess in adult females. However, infection is more severe in children. Most of the cases in adults are a result of odontogenic infections. Also, there is an increase in no of cases due to Pseudomonas species. Increase in the number of multidrug resistant strains is seen. Case of tubercular retropharyngeal abscess is still seen and requires anti-tuberculosis therapy of long duration for complete resolution. Complete surgical drainage of abscess under General Anesthesia reduces duration of Hospital stay.
Modern healthcare facilities with prompt diagnosis and complete surgical drainage under triple antibiotic cover should be promptly available to a child with stridor. Adults need to have better dental hygiene and anti-microbial testing with judicious use of antibiotics. Tuberculosis should always be ruled out in high incidence countries.
Noisy breathing or stridor is a matter of concern in pediatric patients [1]. In adults it presents as neck swelling and swallowing difficulty [2]. Retropharyngeal abscess is a common cause of pediatric stridor, commonly seen in children below five years of age[3]. Etiology might be infective, Traumatic, metabolic, neoplastic or iatrogenic[4]. Infective causes include bacteriological, tubercular, viral and fungal Etiology. Respiratory obstruction is rapidly progressive in children and hence retropharyngeal abscess is invariably fatal until not diagnosed or not drained [5]. Diagnosis may be delayed despite the fact that a retropharyngeal abscess may be diagnosed simply by oral cavity examination and a plain x ray neck lateral view [6]. When suspected, contrast enhanced computerized tomography should be done to delineate it's complete extent and so that complete drainage may be ensured. CT contributes greatly to the diagnosis, but it has limitations in differentiating abscess from cellulitis of the retropharyngeal space.
The plain radiograph in lateral view is very specific when it shows air in the retropharyngeal space [6]. However, steps for radiological and microbiological diagnosis should not delay any step of medical and surgical management as there is a risk of airway obstruction and death. Posterior pharyngeal wall bulge is seen on oral cavity examination [2]. Patients are started on Amoxycillin + Clavulinic acid 30mg/Kg body weight per dose maximum 1.2 gram per dose intravenous thrice daily or Injection Piperacillin + Tazobactum 75 mg/Kg body weight per dose maximum 3.375 gram per dose administered 6 hourly if Pseudomonas is suspected, Amikacin 10mg/Kg body weight maximum 500 mg per dose twice daily, Metronidazole 10mg/Kg body weight maximum 500 mg per dose thrice daily [8]. Plain x ray neck lateral view shows retropharyngeal opacity obstructing airway/food passage/both [6]. Immediate contrast enhanced computerized tomography is done to see extent of abscess in patients where repeat drainage is difficult.
The ideal time to make the drainage is in dispute. Some suggest local antibiotic injection at the same time as surgical drainage. Some studies suggest drainage of retropharyngeal abscess in selected cases only. Intra-oral or external drainage will be done depending on extent of involvement [7]. Procedure should done in General Anesthesia in pediatric patients and uncooperative patients [9]. In other patients, drainage without Anesthesia in sitting position is preferred [10]. Few patients may require external drainage as well [11]. Pus culture sensitivity and AFB should be sent in all patients [12]. Average hospital stay is less than 20 days where intraoral drainage alone is sufficient [13]. But cases with external drainage take more time in healing of surgical wound and duration of stay increases to 1-3 weeks [8]. Rapid recovery is seen in most cases following complete incision and drainage of abscess [14].
This is a multicentric retrospective study conducted at two tertiary care centres at India- PGIMS Rohtak and G S Medical College & Hospital Hapur including data of admitted patients in the Department of ENT over last 3 years (1st April 2019- 31st March 2022)
Patients of all ages, patients of either sex who satisfied all of following criteria were included in the study.
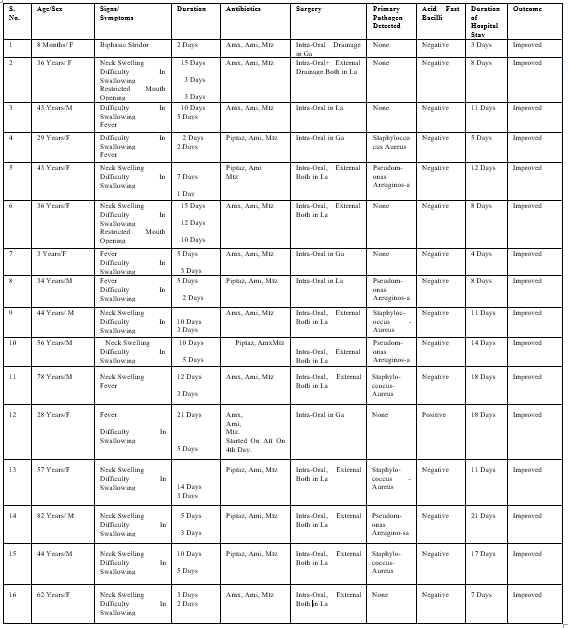
Abbreviations - S. No. - Serial Number,M- Male, F- Female, GA- General Anesthesia, LA- Local Anesthesia, Amx- Amoxycillin Clavulinic Acid, Amk- Amikacin, Mtz- Metronidazole, Piptaz- Piperacillin Tazobactum, all administered intravenously.
We collected data for patients admitted with retropharyngeal abscess at PGIMS Rohtak and G S Medical College & Hospital Hapur from 1st April 2019- 31st March 2022. The data was tabulated in accordance with some significant clinical points and interference drawn regarding diagnosis, treatment approach, morbidity and outcome. Microsoft Windows SPSS 24 package was used to draw following interference.
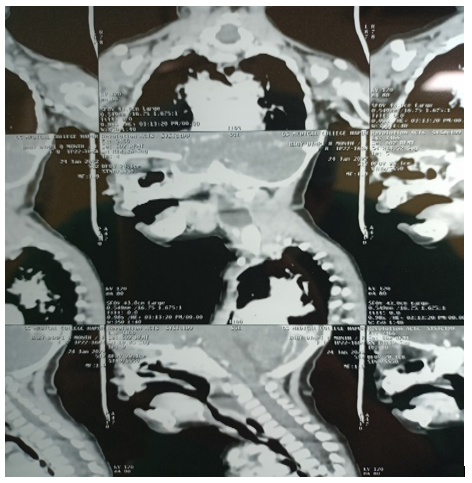

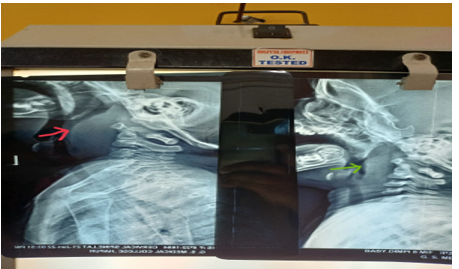
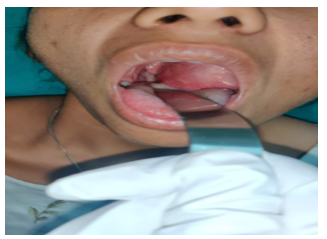
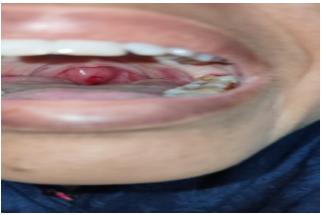

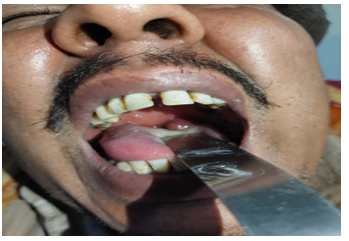

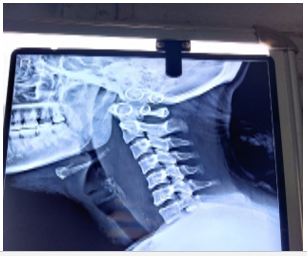
We collected data for 16 patients over 3 years (2 children and 14 adults). First case was an eight months sick child with severe biphasic stridor and massive retropharyngeal opacity (Figure 1.1-Figure 1.3). She was intubated early during presentation and immediate surgical drainage was planned. She underwent a fast recovery and was discharged on second post-operative day. Figure 1.4-1.9 shows other clinical pictures. All the data was tabulated (Table 1.1) and results were drawn.
Majority of patients admitted with retropharyngeal abscess were adults. We saw a female predominant picture (Male: Female ratio 7:9). The cause for infection was antecedent nasopharyngeal infection in pediatric patients. Amongst adult patients (total 14, 11 had odontogenic causes, 5 had diabetes mellitus and one patient had injury by fish bone which he coughed out by himself by frequently gagging with his fingers 5 days back but developed retropharyngeal abscess. In all patients, diagnosis could be made on presentation. In patients with breathing difficulty and inability to swallow, abscess was drained on urgent basis. 6 patients required drainage on urgent basis including both pediatric patients. In three of them surgical drainage was done in GA while in other three patients puncture with 16 Gauze needle and aspiration in LA was done. In other patients also, it was ensured to aspirate pus sample soon on presentation and send it for microbiological culture-sensitivity. Empirically triple antibiotics were started soon after obtaining pus sample. Antibiotics may be changed later as per culture-sensitivity report in poorly responsive cases.
However, no such need was felt in any of our patients. All the patients improved symptomatically with drainage and antimicrobial cover. Improvement was more rapid in patients where complete excision was done in General Anesthesia (within a day) compared to patients where puncture and aspiration in Local Anesthesia was done (1-3 days). Patients with external skin incision were admitted longer (8-21 days) as complete healing took more time compared to patients with intra-oral incision only (3-11 days). Duration of hospital stay was less in patients where surgical drainage in GA was done (3-18 days) compared to those where puncture and aspiration in LA was done (8-21 days). However, the admission day on which drainage was done had no effect on duration of hospital stay.
Retropharyngeal abscess are seen due to infection of deep neck spaces. These deep neck space infections can result in immediate life-threatening emergency, with potential for airway compromise and other catastrophic complications [15]. The retropharyngeal space is posterior to the pharynx, limited by the bucco-pharyngeal fascia anteriorly, the prevertebral fascia posteriorly, and the carotid sheaths laterally. It extends superiorly to the base of the skull and inferiorly to the mediastinum [16]. Bacteriological causes are seen in most of cases and include beta-hemolytic Streptococci and Staphylococcus aureus, anaerobic organisms (species of Bacteroides and Veillonella), or Gram-negative organisms (Haemophilus parainfluenzae and Bartonella henselae) [17]. In our patients, we isolated only two species Staphylococcus Aureus and Pseudomonas Areugenosa.
Retropharyngeal abscess has high mortality as it is capable of complications like airway obstruction, mediastinitis, aspiration pneumonia, epidural abscess, jugular venous thrombosis, necrotizing fasciitis, sepsis, and erosion into the carotid artery[18]. While in children, abscess are because of nasopharyngeal infections, in adults abscesses are usually secondary to dental infections, diabetes and trauma [19]. While retropharyngeal abscesses are considered more common in pediatric patients, we came across more adult patients. The possible explanation is that most of pediatric patients were seen by Pediatrician and ENT consultation was sought for critically ill patients only. Retropharyngeal abscess is more common in males than in females, with generally reported male preponderance of 53–55% [9]. However, we noted a female preponderance (Male:Female ratio 7:9). Adults present with neck swelling, difficulty is swallowing and fever. The most common physical presentation is posterior pharyngeal oedema (37%), nuchal rigidity, cervical adenopathy, drooling, and stridor [19]. Carrying out radiological and microbiological examinations should not delay care [20]. Prompt diagnosis with appropriate choice of antibiotics and surgical facilities wherever required have substantially reduced mortality and morbidity in present era [21].
While children develop retropharyngeal abscess as a result of antecedent nasopharyngeal infections, most of the cases in adults are a result of odontogenic infections followed by Diabetes and trauma. Microbiologically, there is an increase in no of cases due to Pseudomonas species. Increase in the number of multidrug resistant strains is seen. Empirically triple antibiotics should be started after sending pus culture sample and before availability of reports. Antibiotics should be changed as soon as culture sensitivity report is available in poorly responsive cases [22]. Cases of tubercular retropharyngeal abscess are still seen and requires anti-tuberculosis therapy of long duration for complete resolution. Complete surgical drainage of abscess under General Anesthesia reduces duration of Hospital stay.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
