
Research Article | DOI: https://doi.org/10.31579/2637-8892/008
1 The Organization for Promoting Neurodevelopmental Disorder Research, Kyoto, Japan.
2 Graduate School of Medicine, Kyoto University, Kyoto, Japan.
3 Counseling Room, Okinawa, Japan.
4 Kobe Pharmaceutical University, Hyogo, Japan.
*Corresponding Author: Tamaki Amano
Citation: Tamaki Amano, Kumiko Ikemura, Ikuko Amano, Motomi Toichi (2019) Changes in Salivary Biomarkers with EMDR - Evidence for EMDR Effectiveness in Treatment of PTSD, J. Psychology and Mental Health Care. 3(1); DOI: 10.31579/2637-8892/008
Copyright: © 2019 Tamaki Amano, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium,provided the original author and source are credited.
Received: 13 December 2018 | Accepted: 05 January 2019 | Published: 07 January 2019
Keywords: EMDR; salivary stress biomarkers; cortisol; chromogranin A; immunoglobulin A; PTSD
The evidence for EMDR (Eye Movement Desensitization and Reprocessing) ’s effectiveness in treatment usually employs subjective rather than objective measures. Salivary stress biomarkers are considered a useful objective measure of stress. In this study, three salivary biomarkers were examined during EMDR treatment: cortisol (Crti.) as a measure of hypothalamic–pituitary–adrenal (HPA) axis response; secretory immunoglobulin A (s-IgA) as an immune function measure; and chromogranin A (CgA) as a measure of the sympathoadrenal system. Subjects were four adult PTSD (Post-traumatic stress disorder) clients (28–37 years old) who were treated with standard EMDR therapy. Changes in biomarker data during the course of EMDR treatment provided objective evidence for the effectiveness of EMDR therapy. First, Crti. and CgA levels decreased gradually during treatment, indicating that psychological stress was reduced by EMDR therapy. The change in s-IgA was predictably small, showing that the immune system recovered slowly from PTSD. Second, changes in CgA during EMDR sessions reflected the PTSD type (e.g., hyperarousal type or avoidance type) as defined by IES-R subscores. In clients with hyperarousal-type PTSD, pre-EMDR CgA levels were higher than post-treatment levels. Conversely, in avoidance-type clients, levels were lower before than after treatment. These changes were considered to reflect clients’ responses to the requirement that they recall their traumatic memories. The current study successfully shows that changes salivary biomarkers provide physiological evidence of therapeutic mechanism of EMDR in different types of PTSD.
Eye Movement Desensitization and Reprocessing (EMDR) is a form of psychotherapy that has been extensively studied and shown to be effective for the treatment of trauma. EMDR employs a set of standardized protocols that incorporates elements from many different forms of treatment [1]. Usually, to test the effectiveness of EMDR, a therapist uses a combination of two measures during EMDR sessions, the Subjective Units of Disturbance Scale (SUDS) and the Validity of Cognition (VoC) scale. The SUDS was developed by [2], although the version used in EMDR uses a scale of 0–10 instead of the original 100. The SUDS is a measure of current reactivity, with reduced reactivity indicating improvement. This widely used measure has documented validity and reliability, and is correlated with several physiological indices of distress. The VoC scale is an individualized measure of beliefs that was developed by [1]. The VoC uses a semantic differential scale and has documented validity and reliability [3]. The VoC itself has been used successfully in a number of trauma studies. However, both measures are subjective scales that measure clients’ feelings; they are not objective scales. Establishing the effectiveness of EMDR therapy will require considerable objective scientific research in many different fields.
Salivary and blood stress biomarkers are widely considered useful tools for measuring stress. Because saliva collection, unlike phlebotomy, is non-invasive and more acceptable to patients, using salivary biomarkers seems preferable for stress studies [4]. Previous studies of workplace stress, a major cause of anxiety, depression, burnout, and staff turnover, have found that it is correlated with several salivary biomarkers [5]. However, research on psychological stress is complicated because the hypothalamic–pituitary–adrenal (HPA) endocrine system and the immune system interact [6]. The relationship between the nervous system and neuroendocrine responses to stress is mediated by hypothalamic corticotropin-releasing factor, and corticosteroids and catecholamines act as immunosuppressors [7]. Therefore, the choice of salivary biomarker depends on the type of stress being studied. For example, chronic stress is associated with activation of the HPA axis (measured by salivary cortisol (Crti.)) and suppression of immune function (measured by salivary immunoglobulin A (s-IgA)) [8]. Acute stress is associated with activation of the sympathoadrenal system, which is reflected by changes in salivary α-amylase and chromogranin-A (CgA). These are glycoproteins that are co-released with catecholamines (epinephrine, norepinephrine, and dopamine) [9]. The fundamental issue in the psychobiology of a traumatic experiences leading to PTSD is how circulating stress hormones are implicated in the pathogenesis of PTSD [10]. According to classical studies of PTSD (animal experiments) looking at Crti. levels, a cascade of central stress reactions may lead to intrusive recollection of events, avoidance of reminders of events, and symptoms of hyperarousal [11]. In previous EMDR studies, Crti. levels were examined before and after EMDR psychotherapy [12]. However, we considered that the relationship between the sympathoadrenal and immune systems should be examined in PTSD, in addition to the Crti. levels as a measure of HPA axis activity.
In this study, we examined Crti. as the HPA axis hormone indicator, s-IgA as the immune function indicator, and CgA as the sympathoadrenal system indicator in saliva, during EMDR sessions over time.
1. Ethics statement
These experimental procedures were approved by the local ethics committee of the Organization for Promoting Neurodevelopmental Disorder Research, and were carried out in accordance with the principles of the 1964 Declaration of Helsinki. The measures and procedures were explained to all subjects by the examiner, and all agreed and gave written informed consent before the start of the experiment.
2. Subjects
The subjects were four PTSD clients who were treated with standard EMDR therapy. All individuals were adult women (28–37 years old), non-smokers, right handed, and had no neurodevelopmental disorders. One client had Graves’ disease.
Subjects’ saliva was collected at each session. As each biomarker had its own daily variability (circadian rhythm), salivary samples were collected at a fixed time each day. All sessions were conducted in the morning.
Subject profiles
Case 1: Subject A (37 years old, female)
Subject A was the daughter of a lawyer and had a happy life. Her mother had a hysterical personality and often interfered excessively with A’s life. She complained and ordered A to do her best in everything. Eventually the subject became submissive. She was a good and shy student, but chubby. She was often teased by boys, so she started to diet. She became very anorexic and was hospitalized. Her mother sometimes criticized A for neglecting her studies. Consequently, A lost confidence in herself. When she failed her law examination, she tried to commit suicide. She tried several jobs, but could not continue because she had lost her confidence.
Case 2: Subject B (30 years old, female)
Subject B was a policewoman. One day, during working hours, her 22-year-old male colleague killed himself suddenly with his own gun. When B noticed he was missing, she and her colleagues looked for him. They found his body in the forest with a gunshot wound in his forehead. She was the first person to find him, and she was afraid when she saw the blood and the gunshot wound on his face. Because B was his boss, she felt responsible for his suicide. She regretted not having noticed his problems. As a result, she had nightmares of a gun pointing at her forehead just before she was shot. She could not sleep in the dark, so she slept with her room light and TV on. She could not go to work because she was traumatized by the sight of policemen carrying guns. She was absent from work for a year and a half.
Case 3: Subject C (28 years old, female)
Subject C was an excellent student and the captain of a sports team through high school. However, at the university, she could not keep up with her classmates. She finally graduated with a friend’s help. She then got a job, but she was unable to do her job well. Whenever she went to work, she got headaches and vomited. After an absence of a year and a half, she decided to stop working because she lacked confidence in herself. A year later, she got another job, but she could not continue it because her colleagues were unkind and said harsh things to her. Her headache and vomiting recurred, so she took a leave of absence once again. When she recalled these memories, she suddenly became emotional and burst into tears.
Case 4: Subject D (41 years old, female)
This client had experienced many deaths of people close to her. When D was 8 years old, her grandfather committed suicide on New Year’s Eve. When she was 9 and 10 years old, her grandmother and uncle, respectively, committed suicide. Following this, every New Year’s Eve, she would become sick.
Her first panic attack occurred in a car when she was in junior high school. She had no subsequent symptoms for a while, but when she was pregnant with her first child, her panic symptoms reappeared while she was driving. For 10 years, she was treated with psychosomatic medicine, and her condition improved. However, she suddenly had a panic attack again when she took her child to the hospital. Thereafter, every time she heard an ambulance siren, she had a panic attack, so she could not go out alone.
3. Subjective Scales
IES-R is a 22-item self-report measure that assesses subjective distress caused by traumatic events. Items are rated on a 5-point scale ranging from 0 ("not at all") to 4 ("extremely"). The IES-R yields a total score ranging from 0 to 88. Scores for the Intrusion, Avoidance, and Hyperarousal subscales can also be calculated. In general, the IES-R is not used to diagnose PTSD. However, the cutoff score for a preliminary diagnosis of PTSD is 24 [14].
SUDS was used to measure current reactivity in each EMDR session.
4. salivery Biomarkers
Crti., s-IgA, and CgA in saliva were assayed in every session as objective measures. The salivary samples were collected four times during each EMDR session. The first sample was collected before the session (before session). The second sample was collected when the therapist administered the SUDS for before EMDR treatment (pre-EMDR). The third sample was collected at the end of the EMDR treatment (post-EMDR). The fourth sample was collected after the session (after session). The full treatment program took several months.
1.Data development process during full EMDR treatment
As CgA is immediately co-released with catecholamines, the second sample was assayed as data indicating the highest state of arousal. Crti. is secreted into the saliva at a delay of about 30 minutes [15], so the fourth sample was considered to measure the highest arousal. Finally, as s-IgA does not change greatly, the first sample was considered to provide immune data for the day.
2. Data development process during one EMDR session
CgA data are considered to reflect the emotional change process during an EMDR session, as CgA reflects immediate psychic stress levels. CgA levels reflected the amount of catecholamines. However, Crti. and s-IgA were not used to assess changes during individual sessions because they do not change quickly with psychological stress. However, because subject D had Graves’ disease, her CgA data may have been complicated by the influence of thyroid hormones.
Saliva collection
Saliva samples were collected using Salivette® (Sarstedt Co., Ltd., Numbrecht, Germany). Saliva was obtained from cotton that subjects had bitten for 2 min by centrifuging at 3,000 rpm for 5 min. Salivary CgA, Crti, and s-IgA levels were determined by ELISA.
The half-life of these stress biomarkers should also be considered; that of salivary Crti. is about an hour, that of salivary CgA is 15–20 min, and that of salivary s-IgA is 3–5 days. Each sample was stored in an ice box immediately and then stored at -72℃ until the assay.
ELISA assay
To quantify the CgA, Crti, and s-IgA levels, saliva samples were collected and assayed using competitive ELISA kits according to the manufacturers’ protocols. CgA level was determined using a Human Chromogranin A EIA Kit® (Cosmo Bio, Japan); Crti. level was determined using Cortisol, EIA Kit, and DetectX® (Ann Arbor assays, Michigan, USA); and s-IgA level was determined using salivary secretory IgA® (Salimetrics, CA, USA).
Results
1. IES-R
The subjects’ IES-R scores are shown in Table 1, which details the total scores and the scores for the Intrusion, Avoidance, and Hyperarousal subscales. However, subject C did not complete this assessment. In subjects A, B and D, the total scores were >25 (the cutoff point was 24), indicating that the three subjects exhibited PTSD symptoms. At the last EMDR session for subjects A, B, and D all scored below the cutoff point, indicating that their symptoms no longer met the criterion for PTSD. However, subject B’s score was higher during the fifth session than previously, so she continued EMDR sessions for another month. We did not collect saliva samples during the additional sessions.
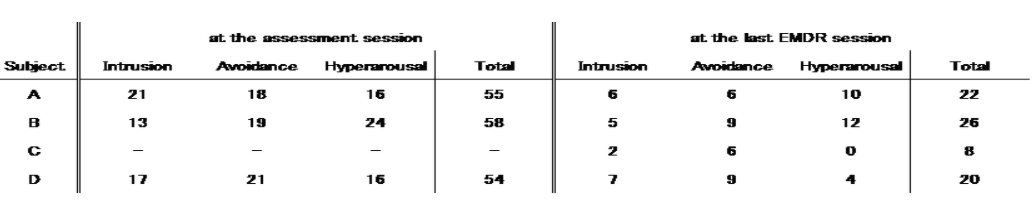
Fig. 1 shows the PTSD types by subscale. Subject A experienced more intrusion than did subjects B and D. Subject B exhibited more hyperarousal than did A and D. Subjects B and D avoided traumatic memories more than subject A did.

2. SUDS score
During the EMDR sessions, the SUDS was used to assess changes in clients’ cognitions. Table 2 shows the subjects’ SUDS scores at each session. In all sessions, the subjects’ SUDS scores decreased enough for them to recover positive cognition. The reductions in SUDS scores indicate the success of each EMDR session.

3. Salivary biomarkers
1) Changes over the full course of EMDR treatment
(1) CgA
Changes in salivary CgA levels are shown in Fig. 2. All levels tended to decrease gradually during the course of treatment.

(2) Crti.
Changes in salivary Crti. levels are shown in Fig. 3. All levels tended to decrease gradually during treatment.

(3) s-IgA
Changes in salivary s-IgA levels are shown in Fig. 4. Little change was observed over the course of treatment.

2) Changes during each individual EMDR session
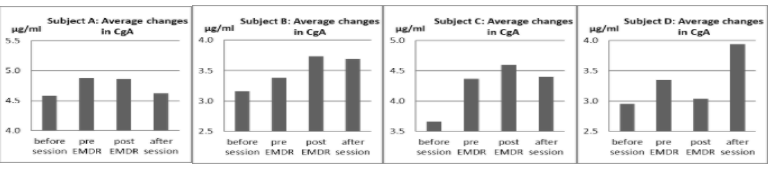
(1) CgA
Changes in the salivary CgA level for each session are shown in Fig. 5. In all subjects, the average CgA level before sessions was low, but it gradually increased during the session. The average level after sessions decreased in all except subject D. As subject D had Graves’ disease, it is possible that her CgA data were complicated by thyroid hormones.
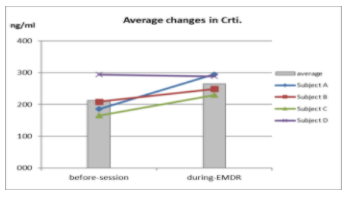
(2) Crti.
Changes in the salivary Crti. levels are shown in Fig. 6. All levels tended to increase during EMDR. This indicates that each EMDR session was more stressful than the pre-treatment period was. This is likely because the subjects had to recall traumatic memories during the EMDR session.
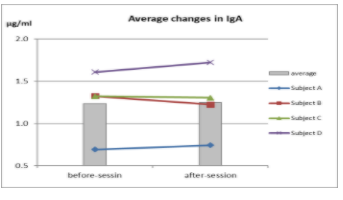
(3) s-IgA
Changes in the salivary s-IgA levels are shown in Fig. 7. There was little change for all subjects, as the immune system does not tend to respond quickly.
Discussion
The data showing changes in IES-R and SUDS suggest that EMDR is effective (Tables 1, 2). They show that the EMDR therapy resulted in a decrease in PTSD symptoms and in negative cognitions. Using subjective indicators, the results indicate that standard EMDR successfully processed the subjects’ trauma.
First, according to objective biomarkers, changes over the full course of EMDR treatment indicated that EMDR therapy was effective. The Crti. levels assayed in the fourth sample and the CgA levels in the second sample were the same as would be predicted under normal physiological conditions because the reflection of Crti. was 30 minutes delayed. CgA and Crti. data (Figs. 2, 3) indicated that EMDR was effective for treatment of PTSD because both levels tended to decrease.
Specifically, in subject A, the CgA and Crti. levels were decreased after the third EMDR session, indicating that EMDR reduced arousal in response to traumatic memories after the third session. In subject B, both CgA and Crti. levels were low during the first session, and both increased gradually after the second session. Both then decreased after the fourth session. As subject B was afraid to recall traumatic memories, she avoided them. In the first session, she was fearful, and her SUDS score dropped from 10 to 8 (Table 2). Her IES-R subscore showed that her avoidance and hyperarousal symptoms were greater than her intrusive ones (see Fig. 1). She was bothered by nightmares and afraid of guns. With EMDR, her fear was focused step by step, and she could finally recall her memory without fear. After her third session, the EMDR effect increased, and her SUDS score decreased from 10 to 3.5 (Table 2). However, her PTSD symptoms remained in the fifth session (her IES-R score was 26). Hence, EMDR was continued for several more sessions, and in the ninth session, her IES-R score was 18 points. Since we could not collect her saliva in the additional sessions, the changes in biomarkers shown here correspond to a point mid-way through her full treatment. After three sessions, both subjects C and D had SUDS scores low enough to indicate that they had recovered their positive cognition. Their CgA and Crti. levels also reflected the effectiveness of EMDR.
As measured by s-IgA levels, there was little change in subjects’ immune systems during EMDR treatment. This suggests that the immune system recovers from trauma slowly. Longer-term research, for several months or years, will be necessary to elucidate this process.
Furthermore, changes measured during each EMDR session also showed interesting results. The CgA results can be classified into two types: In the first type, represented by subjects A and D, pre-EMDR levels were higher than post-EMDR levels; in the second type, represented by subjects B and C, post-EMDR levels were higher than pre-EMDR levels. Clinically, it is easier to focus on traumatic memories with the first than with the second type. Furthermore, the second type suffers more during treatment because it is difficult to focus on the traumatic memories. We considered that these treatment differences were reflected in the IES-R subscores. The Crti. results showed that EMDR therapy was naturally stressful because it was difficult for subjects to recall their traumatic memories (Fig. 6). During EMDR sessions, if a client avoided recalling traumatic memories, it would be impossible to eliminate the conditioned response between the traumatic memories and emotion. In a previous publication, we wrote, ‘one possible mechanism underpinning the main therapeutic stage of EMDR would be as follows: while traumatic memory is activated, induced EMs block the over-representation of the traumatic memory through a forced attentional shift, while they simultaneously ameliorate the conditioned fear by stimulating the AMG’[16]. The present Crti. results indicate success in focusing on traumatic memories, and the CgA results highlight the psychological stress involved in an EMDR session. At first, CgA levels increased gradually as attention was focused on the traumatic memories, and then the stress level was decreased by desensitization through processing traumatic memories during EMDR treatment. With respect to the s-IgA results, as there was little change during EMDR sessions, it appears that the immune system recovers from PTSD slowly (Fig. 7).
Thus, salivary biomarkers were useful in demonstrating the effectiveness of EMDR treatment for PTSD. The use of several salivary biomarkers has recently become a valuable research tool. The current study successfully shows that changes salivary biomarkers provide physiological evidence of therapeutic mechanism of EMDR in different types of PTSD.
This study has several limitations. First, to obtain the data on salivary biomarkers, saliva must be collected at a fixed time because of changes due to the circadian rhythm[17,18]. So, in order to collect saliva in the morning, we were not able to honor all of the clients’ needs in scheduling EMDR sessions. Second, we only tested four subjects. We need to examine more subjects to confirm the present findings, and data should be analyzed using statistical techniques
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
