
Research Article | DOI: https://doi.org/10.31579/2641-0419/248
1,2 Department of Clinical & Interventional cardiology, Apollo Hospitals, Navi Mumbai, India.
3 Department of Cardiology, Lilavati Hospital and Research Centre, Mumbai, India.
4 Department of Cardiovascular and thoracic surgery, Apollo Hospital, Navi Mumbai, India.
5 Department of Cardiac Anaesthesia, Apollo Hospital, Navi Mumbai, India.
*Corresponding Author: Charan Reddy, Consultant, Department of Clinical & Interventional Cardiology, Apollo Hospitals, Navi Mumbai, India.
Citation: Rahul.R.Gupta, K.V Charan Reddy, M.G Pillai, Shantesh Kaushik, Haridas Munde. (2022). Challenges to Transcatheter Aortic Valve Implantation through Femoral Access in Elderly with Peripheral Artery Disease: A Case Report. J. Clinical Cardiology and Cardiovascular Interventions, 5(3); Doi:10.31579/2641-0419/248
Copyright: © 2022 Charan Reddy, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 November 2021 | Accepted: 10 January 2022 | Published: 19 January 2022
Keywords: transfemoral access; multiple co-morbidities; iliofemoral tortuosity or calcification; carotid approach
Transfemoral (TF) access is the safest and the most preferred option for Transcatheter Aortic Valve Implantation (TAVI). However, femoral access is often difficult in a significant number of patients due to inadequate vessel diameter, iliofemoral tortuosity or calcification. Other access routes for TAVI include transapical, transaortic, subclavian, axillary, carotid and transcaval. Choice of vascular access requires both extensive preoperative work-up and adaptive intraprocedural planning by the heart team. Here, we present a challenging case of TAVI in an elderly patient with peripheral artery disease, which required a change in the vascular access site from femoral to carotid artery, midway during procedure, as a strategy to prevent untoward vascular complications. This case also highlights the limitations of current hardware and technologies in negotiating tricky situations.
The concept of transcatheter insertion of heart valves as a treatment option for valvular heart disease was first reported in mid 1960s [1]. It was not until 2000 that the first implantation of a transcatheter pulmonic valve in human was realized [2]. Cribier et al [3] described the first percutaneous transcatheter implantation of aortic valve prosthesis in a 57 year-old patient with calcific aortic stenosis. For a long time the most preferred vascular access for TAVI was transfemoral (TF). However, 10% -15% of TAVI candidates do not have a favorable iliofemoral anatomy for safe transfemoral access [4]. As the technology advances and operator expertise improved, other routes of vascular access in TAVI have emerged. They include transapical, transaortic, subclavian, axillary, transcaval and carotid artery. Lately, transcarotid (TC) is evolving to be the most preferred route in patients in whom TF access is not feasible.
Trans-carotid TAVI was first reported by French group, Modine et al [5] in 2010. Trans-carotid TAVI appears to be safe when compared to other transthoracic access sites with reduced mortality and stroke risk [6]. However, this procedure is not without its inherent risks. The site of access, type, size, and implant position of the transcatheter valve has to be optimized for individual patients with knowledge of echocardiographic and radiographic measurements along with valve haemodynamics and structural anatomy of the vessels. A well planned procedure can prevent peripheral limb ischaemia, valve malposition, coronary occlusion, device underexpansion, and residual aortic stenosis.
Here, we describe a TAVI procedure in an elderly individual with multiple co-morbidities and peripheral artery disease, which necessitated a change in our approach, when encountered with vascular access challenges. This case also highlights various complications that can occur during a TAVI with emphases on planning and flexibility in the thought process, needed to safely complete the procedure.
A 83-year-old female presented with dyspnea on exertion and orthopnea for the last two months. She gives a past history of Diabetes, Hypertension and Coronary artery bypass graft (CABG) surgery done 10 years back with a left internal mammary artery-left anterior descending (LIMA-LAD) and single vessel bypass-right coronary artery (SVG-RCA) grafts. She also gives history of uterine malignancy with abdominal radiation followed by surgery done 30 years back.
Haemoglobin content was 11 gm/dL. Serum creatinine level was 0.94 mg/dL. TTE showed normal Left atrium (LA) and left ventricle (LV) size. LV ejection fraction was 50% with mild hypokinesia of inferior myocardial wall with mild mitral and tricuspid regurgitation. The aortic valve was tricommmisural, stenosed, calcified with indexed valve area of 0.6 cm2/m2. Peak and mean gradients across the aortic valve were 87 mm and 50 mm of Hg respectively. There was no significant valve regurgitation. There was no PAH.
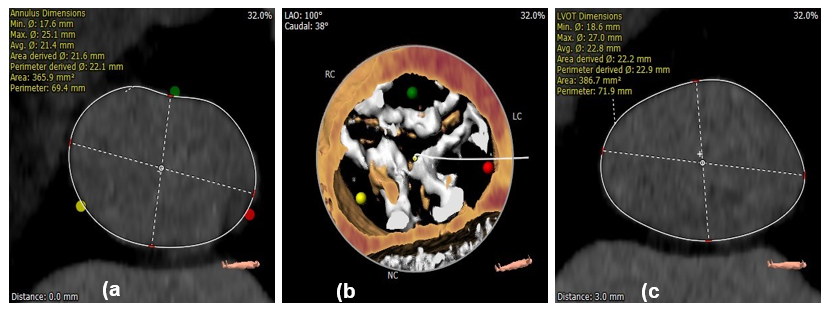
Computed Tomography (CT) based aortogram showed moderate calcification in the aortic valve, ascending arch and descending aorta. The following diameters were measured on CT scan: Annulus (internal diameter) min/max; 17.6/25.1 mm, effective 22.2/22.9 mm (area/ circumference), mid-sinus 28 mm, sino-tubular junction 27.1 mm, height of the left coronary ostium 12.1 mm and to the right coronary ostium 16 mm (Figure-1a-c).
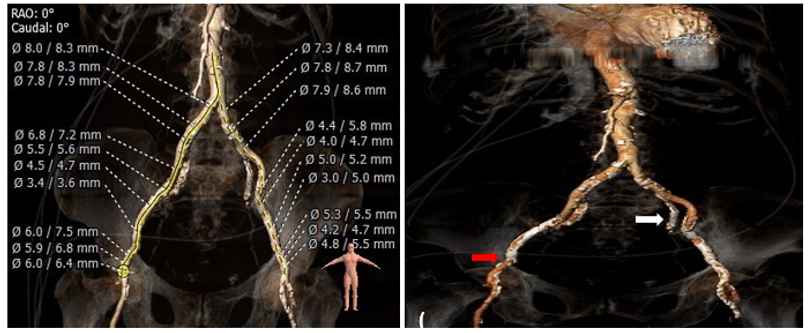
Both common iliac (8.3 mm) and right femoral artery (6.5 mm) diameters were adequate. However, there was a short calcified, circumferential narrowing in the right external iliac artery where the diameter of the vessel was only 3.6 mm. There was a tortuous bend in the left external iliac artery which was also diffusely calcified (4.7mm) (Figure-2a, b).
CT-coronary angiography showed a patent LIMA-LAD and SVG-PDA grafts. It also showed a patent circle of willis with 80% stenosis in the right internal carotid artery. In view of high surgical risk (STS score of 12%) and multiple comorbidities, a TAVI procedure was planned.
During TAVI procedure under local anaesthesia, a 7 French (Fr) sheath was inserted through the right femoral artery (RFA) and two proglide sutures placed in position. The left femoral artery (LFA) pulsations could not be felt and puncture taken did not yield a good blood flow. Hence, a right radial artery was punctured and a 5Fr sheath inserted. A 5 Fr pigtail was advanced into the non-coronary cusp of the aortic sinus using the radial approach. The 7Fr sheath in the RFA was later changed to a 10Fr sheath. However, it could not negotiate the focal narrowing in the external iliac artery (EIA). Shock wave intravascular lithotripsy (IVL) was planned. A designated 300 pulses were given with 7mm x 60 mm IVL balloon catheter at the site of circumferential calcified lesion in the right EIA. Attempts were made to dilate the stenosis, first with 6 mm x 40 mm and later by 8 mm. x 40 mm.
ARMADA balloon was without much success. The lesion site was then stented with a 8 x 60 mm FLUENCY vascular graft. With the help of 14Fr cook sheath, the calcified native aortic valve was dilated with a 18 mm Z-MED II balloon. Inspite of all our attempts the EVOLUT R bioprosthetic valve could not negotiate the stented segment in the right EIA probably due to a calcified spicule or spur at lesion site. As the last measure, the in-line sheath of the EVOLUT R valve was kept proximal to the stented EIA and attempt was made to cross the lower profile EVOLUT R valve across it. This was also unsuccessful and the patient started complaining of severe pain in the right lower leg probably due to vascular insufficiency caused by prolonged procedure.
After consultation with the heart team, a new strategy was devised. Under general anaesthesia and mechanical ventilatory support, the right common carotid artery was exposed with a 4 cm cervical incision and purse string sutures placed. The vessel was sequentially dilated with 7Fr, 10Fr and finally with a 14Fr sheath. A 26 mm EVOLUT R aortic bioprosthetic valve was quickly deployed during rapid right ventricular pacing. The total procedural time was about 7 minutes. Post-deployment angiography, transesophageal echocardiography and aortogram confirmed good valve placement with only a mild aortic paravalvar leak and reduction in trans-aortic gradient to a mean of 4 mm of Hg (Figure.3a-g).

Patient recovered well and was discharged three days later without any permanent lower limb vascular complications. Left subclavian access was not considered due a patent left internal mammary artery (LIMA) graft and the risk of ischemia due to the presence of an occlusive sheath in the subclavian artery. Other transthoracic access sites were not considered due to their invasiveness and their supposedly inferiority over femoral artery access. This case illustrates the importance of planning and anticipation with constant evolution in strategy when facing some seemingly insurmountable obstacles.
Advanced age, female sex, high preoperative New York Heart Association functional class, left ventricular dysfunction, renal failure, pulmonary disease, cognitive impairment, urgency of operation and technical difficulties caused by chest wall adhesions due to previous cardiac surgeries have been identified as predictors of higher operative risk. The development of TAVI has emerged as a lifeline for patients considered being high risk or inoperable providing both an improvement in symptoms and statistically significant mortality benefit.
Retrograde TF access is considered as the gold-standard route for TAVI as it is less invasive and has relatively lower complication rates. However, 10% to 15% of TAVI candidates do not have a favorable iliofemoral anatomy for a safe transfemoral access. The major impediment to a successful TF approach is inadequate vessel diameter, iliofemoral tortuosity or calcification. With the advent of IVL and orbital atherectomy, coupled with availability of newer low profile bioprosthetic aortic valves for implantation, many operators still prefer the age old TF approach, even in diseased peripheral arteries, as they are more experienced and confident with it.
Total of six non-TF access sites are described in the literature. These include the transapical (TA), transaortic (TAo), axillary/subclavian (SC), brachiocephalic, transcarotid (TC), and transcaval approach. No guidelines exist regarding the choice of the first-line alternative pathway if the TF access is not successful, as it is dependent on the patient’s vascular anatomy and operator experience.
However lately, TC route is slowly becoming the choice of access in those patients in whom the TF approach is not feasible or has failed. TC approach allows a direct and shorter pathway to the native aortic valve from the puncture site, with the added benefit of stable catheter delivery and improved movement precision. Several studies have suggested that the TC access might yield better periprocedural and 30-day clinical outcomes than the transthoracic route with outcomes comparable to the TF access [7, 8].
TC access is not without its risks, which include direct injury to the carotid artery, embolic events during vessel manipulation, or transient reduction in blood flow during the procedure leading to transient ischaemic attack (TIA). Hence, a thorough evaluation of atherosclerotic plaques before intervention via appropriate imaging studies (e.g., Doppler ultrasound, with exclusion of patients presenting >50
A growing number of TAVI procedures with standardized pre-procedural diagnostic algorithms and well established intra-procedural steps, has made it a simplified and safe procedure. Transfemoral access remains the most commonly used route for TAVI with low complication rates. With the advent of IVL and orbital atherectomy in the cardiologist’s armamentarium, even unyielding calcified peripheral artery lesions can now be attempted. However, an alternate access site should always be kept ready as a bail-out if TF access is unsuccessful. TC route can be a good alternative to quickly deliver the valve in such difficult cases.
This study was approved by the Ethics Committee of the Apollo Hospital, Navi Mumbai. Informed consent was obtained from the patient.
None
The authors are thankful to the patient for consenting to publish this study. The authors thank all the staff who was involved for making this study for publication.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
