
Research Article | DOI: https://doi.org/10.31579/2768-2757/039
1Pediatric Surgery Unit, Department of Surgery, Enugu State University Teaching Hospital, Enugu, Nigeria.
2General Surgery Unit, Department of Surgery, Enugu State University Teaching Hospital, Enugu, Nigeria.
*Corresponding Author: Chukwubuike Kevin Emeka, Department of Surgery, Enugu State University Teaching Hospital, Enugu, Nigeria.
Citation: Chukwubuike K Emeka, Eze T Chikaodili. (2022). Challenges in the Management of Congenital Malformations in Infants: A Single Centre Experience. Journal of Clinical Surgery and Research. 3(2); DOI: 10.31579/2768-2757/039
Copyright: ©2022 Chukwubuike Kevin Emeka, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 December 2021 | Accepted: 30 December 2021 | Published: 20 January 2022
Keywords: congenital anomalies; challenges; hypospadias; infants; single centre
Background: Congenital malformations are structural anomalies that occur during intra-uterine life that may be identified before or at birth or later in life.
Materials and Methods: This was a retrospective evaluation of the challenges encountered during the management of children with congenital anomalies at the pediatric surgery unit of Enugu State University Teaching Hospital (ESUTH), Enugu, Nigeria. Diagnosis of congenital anomalies was made based on clinical and radiological findings.
Results: A total of 104 infants with congenital anomalies were evaluated during the study period. There was male predominance and majority of the patients were neonates. Seven days and 3 days were the mean age at diagnosis and median interval before presentation respectively. Hypospadias was the most common congenital anomaly and surgical site infection was the most common post-operative complication. Mortality occurred in about one-third of the patients. The general challenges encountered in the management of these patients could categorized as patient related, surgeon related or facility related.
Conclusion:In developing countries, management of congenital anomalies is challenging and is fraught with difficulties. Modifiable factors such as late presentation and provision of facilities will improve outcome.
Congenital malformations also known as congenital anomalies or birth defects refer to structural anomalies that occur during intra-uterine life regardless of its cause. Congenital malformations develop prenatally and may be identified before or at birth or later in life. World Health Organization (WHO) defined congenital anomalies as “any pathological conditions arising before birth, whether they are evident at birth or become evident later in life” [1]. It comprises of a wide range of abnormalities of body structure. The prevalence of congenital anomalies varies widely, ranging from 1.07% in Japan to 4.3% in Taiwan [2]. Among newborn babies, a prevalence of 3 -5% has been reported [3]. The prevalence rate of congenital anomalies may be more in developing countries due to underreporting, unavailability of diagnostic facilities and inaccurate medical records [4]. Congenital anomalies can be correctable or non-correctable. Congenital anomalies may result in lifelong physical and mental disabilities if not managed appropriately and adequately [5]. Treatment of congenital anomalies depends on the specific type of congenital anomalies. In low-income countries, treatment of birth defects can be difficult and challenging due to several factors. There is paucity of data on the challenges experienced in the management of congenital anomalies in developing countries. Toobaie et al reported the lack of robust data on congenital anomalies from low income countries when compared to high income countries [6]. Hence there is need to carry out this study. The aim of this study was to evaluate the challenges we encountered in the management of pediatric patients who presented with congenital anomalies.
This was a retrospective evaluation of the challenges encountered during the management of children with congenital anomalies at the pediatric surgery unit of Enugu State University Teaching Hospital (ESUTH), Enugu, Nigeria. Only children less than 1 year of age with obvious congenital anomalies were recruited into the study. Both elective and emergency cases were considered and this study covered a period of 5 years, from January 2016 to December 2020. Patients who have had surgery for congenital anomalies at a peripheral hospital before referral to ESUTH for reoperation were excluded from this study. ESUTH is a tertiary hospital located in Enugu, South East Nigeria. The hospital serves the whole of Enugu State, which according to the 2016 estimates of the National Population Commission and Nigerian National Bureau of Statistics, has a population of about 4 million people and a population density of 616.0/km2. The hospital also receives referrals from its neighboring states. Information was extracted from the case notes, operation notes, operation register and admission-discharge records. The information extracted included the age, gender, duration of symptoms before presentation, clinical diagnosis, operative procedure performed, complications of treatment, duration of hospital stay and outcome of treatment. Diagnosis of congenital anomalies was made based on clinical and radiological findings. The follow-up period was 12 months. Ethical approval was obtained from the ethics and research committee of ESUTH and informed consent was obtained from the patients’ caregivers. Statistical Package for Social Science (SPSS) version 21 (manufactured by IBM Corporation Chicago Illinois) was used for data entry and analysis. Data were expressed as percentages, median, mean, and range.
Patients’ demographics
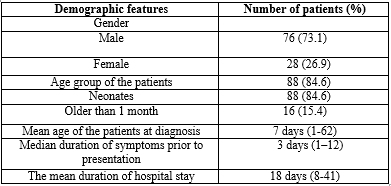
A total of 112 infants with congenital anomalies were managed during the study period. However, 104 infants had a complete record and form the basis of this report. Details of the patients’ demographics are shown in Table 1.
Diagnosis and treatment performed
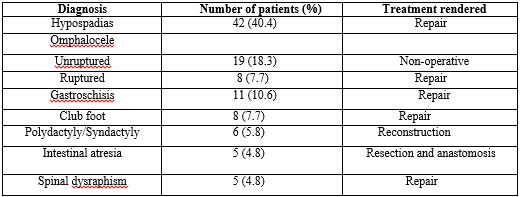
The diagnoses of the patients managed during the study period vary widely. The operative procedure performed was dependent on the type of congenital anomaly. For instance, intestinal atresia was treated by intestinal resection and anastomosis through a laparotomy. Gastroschisis required reduction of the eviscerated bowel and repair of the anterior abdominal wall. The frequency of the different diagnosis and the treatment rendered are shown in Table 2.
Complications of treatment
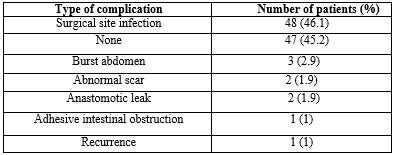
The complications seen in the patients are shown in Table 3.
Treatment outcome
Seventy (67.3%) patients achieved full recovery and were discharged home. However, 34 (32.7%) patients expired. The causes of mortality included overwhelming sepsis 24 (23.1%), respiratory failure 4 (3.8%), anesthesia related death 4 (3.8%) and electrolyte derangement 2 (1.9%).
Challenges of management
The challenges encountered may be patient related, surgeon related or facility/equipment related. It could also be a combination of the various factors.
Congenital anomalies are important cause of mortality and disability. They encompass a wide range of disorders with differing severity [7]. Following the Second World War, the United Nations Scientific Committee on the Effect of Atomic Radiation (UNSCEAR) was empowered to collect and evaluate information on the effect of ionizing radiation on birth defects in children [8]. The setting up this committee demonstrated the importance for epidemiological data on congenital anomalies and the need for surveillance. In the present study, there is male predominance. Other series on congenital anomalies also reported this male predominance [9, 10]. The reason for the gender difference is not known. However, the specific type of congenital anomaly may determine the gender that is more affected. For instance, a study on hypospadias will only involve males. Majority of our patients were neonates. The obvious nature and appearance of congenital anomalies makes them to be detected at neonatal age. Again, severe congenital anomalies present with symptoms that are noticeable at birth. This may explain why several studies on congenital anomalies are carried out on neonates [11, 12]. In fact, Lee et al reported that most congenital anomalies are common in newborns and infants [13]. The mean age at diagnosis of 7 days recorded in the present study is consistent with the report of Ajao et al [14]. A study from Australia reported that 1 out of every 8 case of congenital anomalies is diagnosed in children beyond one year of age [15]. The nature of the congenital anomaly and the presence/absence of symptoms may determine the age at diagnosis. For instance, neonates with intestinal atresia are more likely to be diagnosed earlier than those with intestinal stenosis. The duration of the patients’ hospitalization may be related to the specific pathology, modality of treatment and possible complications that may arise from treatment. Hypospadias was the most common diagnosis in the patients. Other series on congenital anomalies also reported hypospadias as one of the most common congenital anomalies [16, 17]. Hypospadias is a congenital anomaly of the penis in which the urethral opening is not correctly positioned at the tip of the penis [18]. The challenge encountered in the management of children with hypospadias lies in the non-availability of the appropriate sutures required for the repair of the hypospadias. Moreover, most children present with circumcised penis making the hypospadias repair more challenging. Omphalocele was the second most common congenital anomaly managed in the current series. Omphalocele is a midline anterior abdominal wall defect in which there is herniation of the abdominal viscera covered by a thin membrane [19]. Other studies also reported omphalocele as the most common congenital abdominal wall defect [20, 21]. The absence of facilities required for the assessment of chromosomal and other associated anomalies is the challenge encountered in the management of omphalocele. The cost and non-availability of surgical mesh required for repair of the ventral hernia is another challenge. When omphalocele ruptures, it is a surgical emergency requiring immediate operative reduction and abdominal wall closure. This also applies to gastroschisis in which the eviscerated bowel is not covered by membrane. Challenges such as thermoregulation, high risk of infection, nutrition, hypoglycemia and anesthesia are other problems associated with operating on neonate with congenital anomalies. Talipes equinovarus (clubfoot) and polydactyly/syndactyly are congenital musculoskeletal anomalies. Late presentation of children with clubfoot presents a challenge in management due to fibrotic and bone changes that occur in the foot over time. Surgical site infection was the most common post-operative complication recorded in the present study. Ekenze et al also reported wound infection as one of the most common complications in children with surgical correctable congenital anomalies [22]. The high incidence of wound infection may be explained by the large number of neonates involved in the present study. Neonates are not small adults and are prone to infection due to immaturity of the immune system and their low resistance to infections. One-third of our patients died due to surgery related complications. This finding is comparable to the report of a study from Enugu, Nigeria [22]. Severe sepsis in children is detrimental to the wellbeing of the children because it may lead to multiple organ dysfunction syndromes (MODS). Hecker et al documented that post-operative infections cause mortality particularly infants and newborns [23]. Anesthetic complications may lead to respiratory failure and death. One study from Europe emphasized the effect of anesthesia on peri-operative mortality in children [24]. Also, the effect of electrolyte derangements on perioperative mortality in infants has been reported by some authors [25]. Generally, the challenges in the management of congenital anomalies can be categorized into 3: Patient related, surgeon related and facility/equipment related. The patient related factors include late presentation, poverty and nature of the pathology. Surgeon related factors are skill, experience and technique. The facility/equipment related factors are ventilators, incubators, infusion pump and radiant warmers.
1. Only overt (obvious) congenital anomalies were considered.
2. Children older than 1 year of age were excluded.
3. Small number of patients. A larger number would have made better analysis.
In developing countries, management of congenital anomalies is challenging and is fraught with difficulties. Male neonates are mostly affected. Hypospadias was the most common congenital anomaly treated in the index study. Modifiable factors such as late presentation and provision of facilities will improve outcome.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
