
Case Report | DOI: https://doi.org/10.31579/2690-1897/115
Department of Maxillofacial Surgery Hospital of Specialities-Rabat.
*Corresponding Author: Rajaa El azzouzi, Department of Maxillofacial Surgery Hospital of Specialities-Rabat. Faculty of Medicine and Pharmacy-Rabat Mohamed V University
Citation: Rajaa El azzouzi, Othmane Bouanani, Malik Boulaadas. (2022). Cervico-facial Localization of Kimura’s Disease: Two Case Report and Literature Review Journal of Surgical Case Reports and Images 5(4); DOI: 10.31579/2690-1897/115
Copyright: © 2021, Rajaa El azzouzi, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 May 2022 | Accepted: 15 June 2022 | Published: 28 July 2022
Keywords: kimura; parotid tumor; hypereosinophilia
Kimura’s disease is a very rare chronic inflammatory pathology of unknown etiology. It is actually an allergic or autoimmune reaction process involving blood vessels, lymphocytes and eosinophils.
We report a first case of Kimura disease with cervical localization in a 37-year-old male Patient who saw the appearance of a swelling of the right parotid region evolving for 2 years. The patient benefited from a total right parotidectomy, the anatomopathological study of the tumoral piece came back in favor of Kimura’s disease.
A second case of 20-year-old male Patient who saw the appearance of a 3 swelling of the right pre-auricular region, sub mental region and left cheek region evolving for 5 years. The patient underwent a biopsy of submental swelling, the anatomopathological study confirmed the diagnosis of Kimura’s disease. The patient benefited from a Corticosteroid therapy. The evolution was spectacular, with no recurrence at 12 months follow-up.
Kimura’s disease is characterized clinically by subcutaneous nodules of cervicofacial localization, increased volume of salivary glands and satellite adenopathies. Its diagnosis is histological based on the identification of follicular hyperplasia with eosinophilic polynuclear abscesses. Treatment is surgical most often but in some cases Corticosteroid therapy is proposed.
Kimura’s disease is a very rare chronic inflammatory pathology of unknown etiology.
It affects almost exclusively patients from the Far East, but can occur more exceptionally in Caucasian subjects It is characterized by subcutaneous nodules predominating in the head and neck. Its diagnosis is histological. We report a two cases of Kimura disease with cervico-facial localization.
The treatment is not codified but often surgery is used alone as the case of our patient. However, for some cases the indication of general corticotherapy is necessary. The prognosis of the disease remains good.
40-year-old male patient, who consulted for a swelling of the left parotid region, evolving over the last two years, gradually increasing in volume, painful, accompanied by inflammatory episodes with no trismus or facial paralysis of note. The clinical examination found in a patient with good general condition a swelling of the left parotid region with inflammatory signs of the skin, firm of consistency, poorly limited, painful, mobile, measuring approximately 60 mm of long axis. The rest of the head and the neck examination was normal.
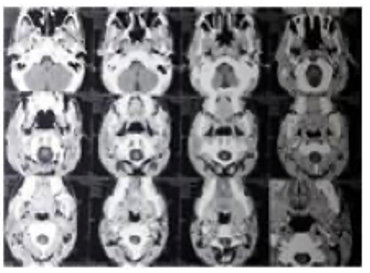
A cervico-parotid ultrasound was requested and revealed an enlarged parotid gland with heterogeneous echostructure. A cervico-facial computed tomography showed an enlarged left parotid gland with irregular contours, infiltrating subcutaneous fat tissue outside, without viewing lithiasic image or bone lysis. CT scan didn’t show any cervical lymphadenopathy.
Cytoponction revealed polymorphic cell inflammation with the absence of suspicious cells.
The biological test found an hypereosinophilia.
We decided to perform a total parotidectomy with an extemporaneous exam. Surgical exploration found an inflammatory-looking gland. The extemporaneous examination was in favor of a non- specific inflammatory reaction made mainly of lymphocytes, with no sign of malignancy. The patient benefited from a total left parotidectomy with no complications. The anatomopathological study concluded with Kimura’s disease.

20-year-old male patient, a Syrian refugee who consulted in our department for the appearance of cervico-facial swellings gradually increasing in volume in 5 years. There were no other symptoms or past medical history of note.
The clinical examination revealed a facial asymmetry due to the presence of swellings of the pre-auricular region, left cheek region and sub mental region, painful, accompanied by inflammatory episodes and melanin pigmentation of the overlying skin, firm of consistency, mobile with measurements varying between 13 mm to 40 mm of long axis, no trismus or facial paralysis associated (Figure 3).
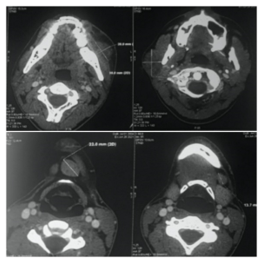
A cervico-facial CT scan was performed, revealing the presence of heterogeneous retro-parotid, pre-mandibular and submental tissue formations. (Figure 4). The patient underwent a biopsy of submental swelling, the histopathologic evaluation and the immunohistochemical profile evoked an eosinophilic lymphadenopathy that may be part of kimura's disease.
blood tests showed an hyper eosinophilia at more than 30% of the white blood cell formula and markedly elevated serum immunoglobulin E levels.Which retains the diagnosis of Kimura’s disease.Biological test and renal ultrasound scan has been completed, returned normal.
The patient benefited from a Corticosteroid therapy. The evolution was spectacular with disappearance of all the swellings after 3 months (Figure 3).

Kimura’s disease (KD) has been considered as a distinct pathologic entity that was first described in 1937 by Kimm and Szeto in China as “eosinophilic hyperplastic lymphogranuloma” and has been known most often as Kimura’s disease since its description by Kimura et al. in the Japanese literature in 1948 [1].
The majority of the cases were reported in Asia, mainly in China, Japan, and Southeast Asia, and were usually seen in young men with unilateral involvement [2], and rarely seen sporadically in non-Asian population [3].
Kimura’s disease can occur at any age, with a peak in frequency in the third and fourth decades, with a sex ratio varying according to studies from 3 to 7 [3,4].
The exact cause and pathogenesis of Kimura’s disease are still unclear, After considering that Kimura’s disease belonged to the tumor group of the vascular endothelium and that it could, as such, be assimilated with angiolymphoid hyperplasia with eosinophilia in Western patients. Today it is thought that it is actually an allergic or autoimmune response triggered by an unknown persistent antigenic stimulus involving blood vessels, lymphocytes and eosinophils.
Kimura’s disease follows an indolent clinical course and misdiagnosis is common, is generally benign and self-limited. Most patients have a prolonged course with gradual increase in the swelling. Occasional spontaneous resolution is seen.
The most common clinical feature is asymptomatic unilateral soft-swelling, such as salivary glands and local lymph nodes, it presents predominantly as subcutaneous nodules in the head and neck, often unilateral, and frequently associated with regional lymphadenopathy with or without the involvement of salivary glands, Sometimes bilateral involvement is also seen as illustrated by our observations. Orbit, eyelid, palate, and pharynx have also been reported to be involved, in addition to the axilla, groin, and arm [5,6]. Epitrochlean, axillary, inguinal and popliteal localizations are described [7].
Radiological examinations can be useful in the exploration of Kimura’s disease, it is helpful for determining the location and extent of pathological changes and lymph node involvement but has low specificity.
Ultrasound examination often shows hypoechoic masses, unclear borders, irregular shape, and uneven internal echo. Some characteristic imaging findings favoring Kimura’s disease are the appearance of ill-defined subcutaneous masses, which are homogeneously isodense to hypodense without necrosis, calcification, or cystic degeneration on CT. On MRI, these masses appear hypointense to isointense on T1-weighted images and hyperintense on T2 images [8,9].
The diagnosis of Kimura’s disease is based on pathological features and elevated immunoglobulin E levels, blood hypereosinophilia is also frequently found. Systematically, a proteinuria that will witness a nephrotic syndrome should be investigated.
Pathological examination is the golden standard for the diagnosis of KD.Some of the most common findings are listed as ‘constant features’, including intact nodal architecture, extensive reactive lymphoid infiltrates, postcapillary venule proliferation, and infiltration with numerous eosinophils accompanied by mast cells, histiocytes, and Langerhans cells. Some other less common features are described as ‘frequent features’, which are sclerosis, polykaryocytes, vascularization of the germinal centers, proteinaceous deposits, necrosis of the germinal centers, eosinophilic abscess, and a reticular IgE deposition within germinal centers. However, none of the above features are pathognomonic for KD: they can be found in numerous other benign and malignant disorders, including angiolymphoid hyperplasia with eosinophilia (ALHE), Hodgkin’s lymphoma, angioimmunoblastic T-cell lymphoma, Langerhans cell histiocytosis, florid follicular hyperplasia, Castleman’s disease, dermatopathic lymphadenopathy, allergic granulomatosis of Churg–Strauss syndrome, lymphadenopathy of drug reactions, and parasitic lymphadenitis [10], hence the interest of clinical-biological and radiological correlation.
Treatment of KD is mainly for cosmetic reasons or for the preservation of functioning while preventing recurrences.The optimal treatment of KD is controversial due to lack of large-scale systemic clinical studies on different treatments for KD, different therapeutic modalities have been proposed.
Surgical excision may be considered the golden standard of treatment for KD especially for the localized lesion, As KD is benign, surgical resection does not spread lesions, but helps to reduce lumps and benefits diagnosis. However, KD typically involves subcutaneous tissue without well-defined boundaries, making it difficult to achieve a negative margin by surgical excision alone and recurrence is possible [11]. Corticosteroid therapy is indicated in forms profuse or inaccessible to surgery or systematically in case of renal impairment. It is prescribed at the initial dose of 0.5 to 1 mg/kg/d prednisone with a slow degression over at least 6 months with good efficacy. However relapses are possible when treatment stops Local radiation therapy may be offered in forms refractory to corticosteroids or when surgery is impossible. Systemic chemotherapy based on 5-fluoro-uracil and azathioprine was used in combination with general Corticosteroid therapy, but its usefulness was not formally demonstrated [12].
We reported in our observations the two scenarios, in the first case the surgical option was preferred in front of the localized form and we opted for corticosteroid therapy in the second case as it’s a disseminated form of KD, in both cases the remission was complete with a mean follow up of 2 years.
KD is a benign disorder characterized by subcutaneous soft tissue masses or lymph-node enlargement with an indolent clinical course. The relevance of those cases is due to the rarity of the disease which mimics neoplastic conditions. Knowledge of Kimura’s disease will put the physicians in a better position to diagnose and treat the disease.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
