
Case Report | DOI: https://doi.org/10.31579/2692-9562/070
1 Sourabh Padmanabhan is Senior Resident. Department of Otorhinolaryngology, Head and Neck Surgery, Gandhi Medical College and Hospital, Secunderabad, India.
2 Mounika Reddy Y is Assistant Professor. Department of Otorhinolaryngology, Head and Neck Surgery, Gandhi Medical College and Hospital, Secunderabad, India.
3 Moota Madhuri is a final year post graduate. Department of Otorhinolaryngology, Head and Neck Surgery, Gandhi Medical College and Hospital, Secunderabad, India.
4 Shobhan Babu A is Professor and Head of the Department. Department of Otorhinolaryngology, Head and Neck Surgery, Gandhi Medical College and Hospital, Secunderabad, India.
*Corresponding Author: Mounika Reddy Y, Department of Otorhinolaryngology, Head and Neck Surgery, Gandhi Medical College and Hospital, Secunderabad, India.
Citation: Sourabh Padmanabhan, Mounika Reddy Y, Moota Madhuri, Shobhan Babu. (2023). Cervical Scrofula Mimicking Thyroid Malignancy: A Rare Presentation with Pretracheal Lymph Node Involvement in an Adult Female, Journal of Clinical Otorhinolaryngology, 5(3); DOI: 10.31579/2692-9562/070
Copyright: © 2023 Mounika Reddy Y. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 14 January 2023 | Accepted: 30 January 2023 | Published: 01 February 2023
Keywords: scrofula; pretracheal lymph node; extrapulmonary tuberculosis; tb lymphadenitis
Cervical lymphadenitis is the most common extrapulmonary manifestation of TB. Here we report a rare case of cervical scrofula (TB lymphadenitis) involving the pretracheal lymph node. It is essential to undergo a proper radiological assessment to differentiate between thyroid nodule and lymph node pathology and thus avoiding surgical intervention.
Pretracheal tubercular abscess is a rare presentation of extra pulmonary tuberculosis.[1] It usually presents in posterior triangle group of lymph nodes.[2]
A 33 old female patient presented to our otolaryngology outpatient department complaining of mild pain and a swelling over the anterior aspect of her neck that had been present for a month. She also gave history of rupture of swelling. Patient had no complaints of evening rise of temperature, cough, dyspnoea, dysphagia, change in voice and foreign body sensation in the throat. She had similar complaints of left sided neck swelling 2 months back which subsided with antibiotics. Not a known case of diabetes, hypertension, coronary artery disease, cerebrovascular accidents, tuberculosis (TB), asthma, thyroid disorders, seizures, genetic disorders and no past surgical interventions.
Clinical examination of the neck, revealed an oval swelling of size 1x2cm, involving the anterior part of the neck, 1cm above the suprasternal notch. A discharging sinus was visualised over the swelling. Skin over the swelling showed signs of inflammation and the swelling did not move with protrusion of the tongue or on deglutition. Vitals and all routine investigations were normal. ESR was 114mm after 1st hour. Thyroid profile was normal. On further evaluation, ultrasonography (USG) of the neck showed TIRADS 4 isoechoic soild lesion involving the right lobe of thyroid indicating suspicous of malignancy. USG also revealed multiple bilateral level IV, VI, supraclavicular nodes with loss of fatty hilum with the largest measuring of 1cm x 0.8cm. Discontinuity was noted in the level VI lymph node with evidence of 1.6cm x 1cm collection in subcutaneous plane on anterior aspect of neck showing communication in above mentioned lymph node suggesting a ruptured cyst. As all these features were favouring towards thyroid malignancy, further investigations were done. A USG guided fine needle aspiration cytology (FNAC) of the swelling in neck was suggestive of benign follicular nodule- BETHESDA Grade-II. As all these investigations were still inconclusive to reach a confirmatory diagnosis Magnetic resonance imaging (MRI) of the neck with gadolinium was done. On MRI, T2 weighted STIR sequence revealed aa ill defined peripherally enhancing hyperintense collection in the intermuscular and intramuscular planes just adjacent to the insertion of right sternal head and was extending into the cutaneous plane with a skin breach in the suprasternal region. MRI T2 weighted STIR also showed multiple hyperintense small peripherally enhancing collections with adjacent marrow edema within the manubrium, body of sternum, right transverse process of C7 and right supraclavicular lymph nodes. There were cortical breach noted in the anterior aspect of the manubrium and right transverse process of C7. Altered signal intensity was noted in the vertebral bodies of D2, D3 with anterior cortical breaks with a peripherally enhancing T2-STIR hyperintense collection measuring 3.3×1.7×1.9cm in prevertebral space (Figure 1). All these features were suggestive of infective spondylitis most probably of Koch’s etiology. To confirm the diagnosis, discharge from the swelling was sent for acid fast bacilli, which turned out to be positive. Further CBNAAT was also positive for Mycobacterium Tuberculosis and was sensitive for rifampicin. Patient was started on ATT.
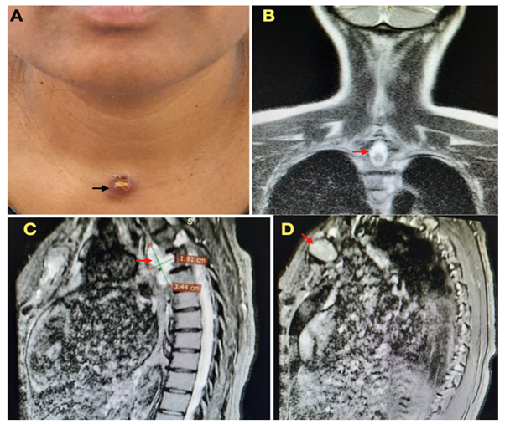
Figure 1: (A). Clinical image showing swelling infront of the neck with a discharging sinus (black arrow). (B,C,D). MRI neck, T2 weighted STIR squence (B). Coronal view, (C,D). Saggital view showing hyperintense collection (red arrow) in the neck (B,D) and in the pre vertebral space (C).
Tuberculosis is still the most prevailing disease in countries like India contributing to 22.7% of the global burden. Lymph node involvement is the most common presentation of extrapulmonary disease. Cervical group (60–90%) of lymph nodes are most commonly involved.[3] Reported literature has shown that TB lymphadenitis is most commonly involves the posterior triangle group of lymph nodes.2 Posterior triangle nodes accounts for 51% [3] followed by upper deep cervical and submandibular nodes. Pretracheal tubercular abscess is a very rare presentation of extrapulmonary tuberculosis accounting for less than 1%.[1] Anterior group of nodes is very rare accounting for <1>
Most of them are seen to present in the stage of lymphadenitis[4,5] as single or multiple painless swellings. Most of the times it spreads through the primary focus in the lungs, tonsil, adenoids or via contiguous spread from the mediastinal, peri bronchial nodes or adjacent group of nodes. Presentation of the anterior group of lymph nodes classically mimics a thyroid nodule or thyroglossal cyst due to the location of swelling and signs associated with it.[6] Swellings anatomically located in the area of anterior group of lymph nodes should be dealt with high degree of suspicion for tubercular etiology especially in TB endemic areas (WHO, 2014 ).[3]Radiological findings of hyperintense collections on T2W STIR, with proven positivity for Acid Fast Bacilli on AFB stain and CBNAAT confirmed a presentation of tubercular abscess. With great advances in imaging and laboratory investigations the patient was confirmed with a diagnosis of Extrapulmonary Tuberculosis and was started on a course of anti tuberculous treatment Category 1 for 6 months as per RNTCP- Guidelines for TB control in India. Patient was also counselled and asked to watch for complications of anti tuberculous drugs.
A proper radiological assessment is of utmost importance to differentiate between thyroid nodule and lymph node pathology. A possibility of extrapulmonary lymphadenitis and should be considered as a differential diagnosis in all cases of TB lymphadenitis. Adequate evaluation will avoid major surgical intervention in cases for an infectious pathology like tuberculosis.
The authors would like to gratefully acknowledge and thank medical supernindent, faculty, postgraduates, patients and attendants for accepting for publication.
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent was obtained from all patients included in the study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
