
Research Article | DOI: https://doi.org/10.31579/2578-8868/125
1* Neuropsychiatry Specialist, Abbassia Psychiatric Hospital, Cairo, Egypt.
*Corresponding Author: Andrea Ascoli Marchetti, Vascular Surgery Unit. Biomedicine and Prevention Department. University of Rome Tor Vergata. Viale Oxford 81 00133 Rome Italy.
Citation: Ascoli Marchetti A., Oddi F.M., Battistini M.,De Liso A.,Testa A, Pallocchi M., Ippoliti A. (2020) Cervical manipulation and cerebrovascular ischemia. A rare but dangerous association. Monocentric experience in a high CEA volume center and literature review. J. Neuroscience and Neurological Surgery. 6(4); DOI:10.31579/2578-8868/125
Copyright: © 2020 Andrea Ascoli Marchetti, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 27 June 2020 | Accepted: 09 July 2020 | Published: 14 July 2020
Keywords: cerebral ischemia; carotid surgery; neck manipulation; cervical spine; emergency surgery; artery dissection; vascular surgery volume center; cervical trauma; cerebrovascular insufficiency; acute carotid plaque; cervical manipulation; rehabilitation
Background: A correlation between stroke and cervical manipulation in the neck is reported in the literature with increasing frequency, and each new publication seems to rekindle the debate. The manipulations in the cervical region is potentially dangerous for arterial vessels. The aim of this work is to analyze the incidence of these events in the experience of a center with high volume surgery, in which emergency interventions are performed for acute cerebrovascular Ischemia.
Methods: Data were collected regarding patients undergoing carotid endarterectomy surgery for neurological symptoms of cerebrovascular insufficiency over a seven-year period.
Results: The intervention was conducted urgently in 66 cases for acute symptoms (7.6%) with a median symptom interval / CEA: 39.4 ± 5.4 h) in 32 cases for hemispheric transient ischemic attack, while in 34 for minor stroke. Only in 1 case (1.5%) did a condition of severe spondyloarthrosis of the cervical spine occur in acute carotid plaque in C4-C5. In another case (1.5%) a cervical trauma caused by beatings is documented.
Conclusions: Manipulations of the neck and cervical spine can rarely cause or contribute to worsening neurological symptoms, however they should always be considered.
The manipulations of the cervical spine and neck, performed by the physiokinesitherapy specialist or as a part of assault, involve a maneuvers which may influence the carotid and vertebral arteries [1]. A correlation between stroke and cervical manipulation is reported in the literature with increasing frequency. Specific risk factors related to cerebrovascular complications following manipulation of the cervical spine have not yet been identified [2]. for this reason, each patient is to be considered susceptible to this risk, especially if over 45 [3]. Patients undergoing spinal manipulative therapy must, therefore, informed of the possible risk, express a consent, aware of the possibility, albeit remote, of stroke or vascular lesions [4].
Materials and Methods
Institutional review board approval for the study and written informed consent from all patients or surrogate decision-makers were obtained. A retrospective analysis of prospective data collected from consecutive patients with TIA or ischemic stroke admitted to the hospital between October 2012 and December 2019 was analyzed. We collected 873 carotid endarterectomy (CEA) operations. Of these surgical procedures, 66 (7.6%) were conducted in an emergency for acute neurological symptoms (median symptom interval / CEA: 39.4 ± 5.4 h), in 32 cases for hemispheric transient ischemic attack (TIA), while in 34 for minor stroke. Color duplex ultrasound (US) imaging and/or multislice computed tomographic (CT) angiography examination were employed to define the site, length, and degree of stenosis as well as the structure of the carotid bifurcation morphology. An ischemic stroke was defined as any new, persistent neurologic deficit caused by disturbances in the blood supply to the brain with acute infarction visible on MRI or CT scan. Selection criteria for a possible extracranial revascularization procedure were the presence of an atherosclerotic carotid artery lesion located on the clinically relevant side with a stenosis of 70% or an unstable 50%–69% stenosis (i.e.: ulcerated lesions and/or thrombus in the lumen) [5-6].
Only in 1 case (1.5%) did a condition of severe spondyloarthrosis of the cervical spine occur in acute carotid plaque in C4-C5 (Figure 1).
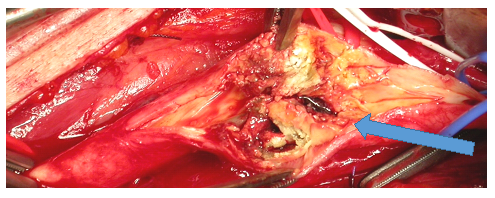
In another case, CEA was performed in a patient with an ischemic stroke and floating thrombosis in dissection of the common carotid artery after cervical trauma caused by beatings (Figure 2) [7].
The results of our urgent case studies are in line with those reported in the literature [8]. The 30-day IMA/stroke rate was 7.6% (5 cases), with a mortality rate of 1.8%. In 53.1% of cases, we reported an improvement in neurological deficits. At follow-up (FU-mean of 22 months, with interval 3-39), we observed 2 carotid restenosis (3.1%) and a new neurological deficit in 4 cases (6.1%).
Etiology
It is well known that in chronic inflammatory rheumatic diseases, systemic inflammation can act independently or in synergy with traditional cardiovascular risk factors, contributing to the development of cerebrovascular complications [3]. and Gonzalez-Gay et al. [9], studied 64 ankylosing spondylitis patients and documented a greater carotid myointimal thickness (IMT) and a higher frequency of atrophic carotid plaques than the control population. To date, numerous absolute and relative contraindications to the FKT maneuvers to treat these arthritic patients have been identified. Patients with severe herniated discs are exposed to greater risks of cerebrovascular complications during these practices. [10]
In 1934 the first scientific-legal work was published on the detection of cerebrovascular accidents after manipulation of the spine. In a recent paper Thomas and colleagues report the manipulation of the neck as a risk factor for dissection in cervical area [11]. The proximity of the vertebral artery to the vertebral bodies (in C1 and C2) can play a crucial role in the development of dissection. The greater mobility compared to the anatomical planes of the vertebral artery in V1-V2 can also be a favoring factor for stretching injuries [12]. To confirm this hypothesis, segment V3 is the most frequent site where dissection takes place However, dissections are also described in other segments of the vertebral artery. Dissection of the carotid artery is rarer during chiropractic maneuvers, probably because it is surrounded by soft tissues and less contiguous with the bone planes. For this reason, carotid dissection is presumed to result from compression of the artery against both transverse processes or against the soma of the cervical vertebrae, as in our previous described case [7]. The pharyngeal segment of the internal carotid artery, extending from the carotid bifurcation to its entry into the petrous portion of the temporal bone is less mobile, and therefore more susceptible to injury. Although these adverse events tend to be self-limiting, serious cerebrovascular adverse events, such as TIA and stroke, are reported in various series in the literature (Table 1).

More specifically, lesions such as dissection of the common, vertebral, internal carotid artery, or vertebrobasilar segment have been found following manipulation of the cervical spine. ). Sports, assault and road accidents are the principal etiology for blunt trauma of the neck and no definitive management guidelines regarding this type of injury exist, our reports emphasizes the role of conservative anticoagulation therapy in the management of this rare condition, on the contrary in our experience, the approach was surgical. [13].
Physiopathology
Shari W et al. confirm with their study the rarity of cerebrovascular events following physiotherapy maneuvers. Of these events, 70% are vertebral artery and carotid dissections [12]. These injuries are due to intimal laceration related to excessive stretching of the artery during rotational manipulation. This seems to occur more commonly on the wall of the vessel which runs at the atlanto-epistrophe joint. Intimal injury can be followed by hemorrhage, pseudoaneurysm, intramural formation, resulting in thrombosis, embolism or arterial spasm. Currently, in consideration of the possible complications related to cervical manipulations, some physiotherapists require pre-treatment diagnostic screening in those patients who have cardiovascular risk factors. In fact, based on post-mortem studies on human vertebral arteries, Cagnie et al. [14] have suggested that, in the presence of atherosclerotic alterations, the maneuvers of elongation of the spine and the compression effects related to rotational manipulations of the head represent a concrete risk factor for the aforementioned vascular lesions. Therefore, therapists should avoid performing manipulative techniques at all levels of the cervical spine in the presence of any direct or indirect signs of atherosclerotic disease or in the presence of calcified or tortuous arteries [15-17]. Sports, assault and road accidents are the principal etiology for blunt trauma of the neck and no definitive management guidelines regarding this type of injury exist, our reports emphasizes the role of conservative anticoagulation therapy in the management of this rare condition, on the contrary in our experience the approach was surgical [18,19].
Diagnosis.
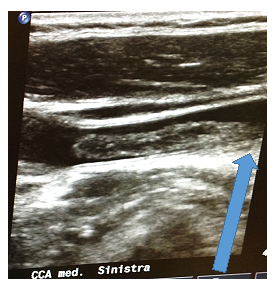
The ecocolordoppler is considered the gold standard in identifying lesions of the epiaortic vessels in their extracranial course [17]. The ecocolordoppler allows determining the direction of the blood flow (i.e., anterograde or retrograde), using the color and flowmetric method, which is particularly useful in identifying lesions upstream and downstream of the extracranial traits that can be explored and in determining a functional assessment of intracranial circulation. Particularly useful in the evaluation of proximal subclavian stenosis with subclavian steal syndrome. In addition to the directional information, the ultrasound method can provide flow velocity and therefore to allow hemodynamic analysis of any vascular lesion [17]. Unfortunately, this instrumental method has as its limit the precise morphological evaluation of the vertebral arteries in its ostia and intracranial features. Normal flow in the vertebral artery is typically pandiastolic, because the supply is for a low resistance vascular bed (LR). A high-resistance signal (HR) in vertebral territory with the loss of the characteristic diastolic flow, may indicate a more distal vertebrobasilar lesion. Magnetic resonance imaging (MRI) and CT angiography (CTA) offer potential advantages for the non-invasive assessment of vascular lesions; in particular, they have proved to be useful for the evaluation of dissections (Figure 3 a, b) [13,19,20].

Typically, the most used magnetic resonance imaging (MR) techniques for the evaluation of arterial dissection include T1-weighted images (T1WI), T2-weighted images (usually with spatial presaturation), with or without fat suppression, and magnetic resonance angiography (MRA). In particular, the diffusion sequences (T1WI) can provide direct visualization of intramural hematoma, even if subacute. T1-weighted images (3D - BB - T1WI) can also improve the evaluation of intramural hematomas, further completing the diagnostic evaluation. The MRI appears the gold standard in early thrombectomy protocols, when intracranial vessels are involved [19].
Treatment
Dissections, if diagnosed, are managed through conservative treatment, involving the use of anticoagulants (21). The prognosis of medical treatment is generally favorable, where it concerns self-limiting lesions. Surgical or endovascular revascularization is reserved for patients with persistent or recurrent symptoms that do not respond to anticoagulant therapy (7). As for medical therapy, there is no evidence from randomized studies (21-22) to determine whether, in carotid dissections, the use of antiplatelet therapy is superior to anticoagulant therapy. Endovascular interventions conducted for the treatment of cerebral ischemic complications following the dissection of epiaortic vessels represent an effective method especially in the case of distal lesions. These interventions are represented by mechanical thrombectomy and stenting of intracranial vessels. Stenting of the carotid or vertebral artery has been reported in patients with recurrent embolism, hemodynamic stroke, or in case of a volumetric increase in pseudo-aneurysmal lesions. Besides, stenting on dissection, followed by intra-arterial infusion of thrombolytic agents, is considered a further therapeutic chance in the selected cases, where acute thrombotic occlusion phenomena of dissecative lesions or in the case of intramural hematomas complicated by thrombotic events are concomitant. In the event of phenomena of acute thrombosis affecting the common carotid and internal extracranial carotid artery, mechanical thrombectomy and stenting or thromboendoarterectomy of carotid bifurcation are reported, where, even if there are no bleeding or distal thrombotic complications, according to the study protocols implemented with the Stroke Unit (23).
Patients with carotid or vertebral atheromasia associated with chronic inflammatory disease of the spine seems to present a higher risk of cerebrovascular complications, but further analysis should be necessary to establish the exact role in cerebrovascular disease. An adequate diagnostic screening to prevent possible vascular cerebrovascular complications in patients with cardiovascular risk factors, should be done, before manipulations of the cervical spine. In case of assault the carotid axis is anatomically predisposed to dissection and in case of neurological symptoms a diagnostic evaluation should be done.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
