
Research Article | DOI: https://doi.org/10.31579/2578-8965/153
Department of Obstetrics and Gynecology, Faculty of Medicine, Ain Shams University, Egypt.
*Corresponding Author: Beshoy N. Dawood, Department of Obstetrics and Gynecology, Faculty of Medicine, Ain Shams University, Egypt.
Citation: Alaa M. Atef, Karam M. Bayoumy, Beshoy N. Dawood, Mohamed A. Abdelhaleem, (2021), Cervical and Lower Uterine Thickness Ultrasound Examination for Prediction of a Successful Induction of Labor. J. Obstetrics Gynecology and Reproductive Sciences, 5(9) DOI: 10.31579/2578-8965/153
Copyright: © 2021 Beshoy N. Dawood, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 December 2021 | Accepted: 14 December 2021 | Published: 29 December 2021
Keywords: cervical/lower uterine thickness; ultrasound; induction of labor
Background: Modern obstetrics inducts 20% of all deliveries. Because not all inductions result in a vaginal birth, finding the best way to predict success is essential. The lower uterine segment thins with gestational age. B-mode ultrasonography detects this. Measuring the LUS myometric thickness quantifies the risk of uterine rupture during vaginal delivery following a cesarean section. Aim of the Work: to evaluate different sonographic characteristics for the cervical and lower uterine segments in in order to predict labour induction and vaginal delivery. Results: Induction was successful in majority of cases (96.2%). Mean±SD of Time until active phase and delivery was 4.1±2.7 and 7.6±3.1 hours respectively and Normal vaginal delivery was the most frequent mode in majority of cases (93.3%). Cases with successful induction statistically had non-significant higher Effacement and Bishop Score, but had significant lower cervical length and LUS thickness and so higher Manipal score. Conclusion: we were able to present data that cervical structural changes occurred at the internal OS level, i.e., shortening through funneling. These structural changes may be the determining factor for successful induction of labour.
One of the most frequent procedures in modern obstetrics is induction of labour, which accounts for 20% of all deliveries (Kehila et al., 2016). Choosing the most effective strategy to predict successful labour induction and vaginal birth is crucial because not all of these inductions result in a vaginal delivery (Cubal et al., 2013).
The Bishop score is a common measure for determining whether an induced labour will end in a successful vaginal birth, however, evaluation is subjective and a poor indicator of how labour induction will turn out (Feghali et al., 2015), especially when the external OS is closed (Kim et al., 2020). In the obstetric community, there has been huge attention in the prediction of a successful induction of labour (IOL).
Measurement of cervical length and the prediction of successful IOL are under question. Yet, its sensitivity is significantly higher than the Bishop score (Zhou et al., 2016).
Lower uterine segment (LUS) weakening occurs as gestational age increases (Kok et al., 2013). This can be detected using B-mode ultrasound.
To our knowledge, no study has looked at the myometrial thickness or the consistency of the LUS in relation to successful IOL or the onset of labour (Hamza et al., 2021).
Bishop score and uterine cervical length are regarded as reliable indicators of a successful labour induction. An increased rate of failed induction is seen when the Bishop score decreases (Bishop, 1955, Chung et al., 2015).
Transvaginal ultrasonography-measured cervical length has recently become a commonly used clinical index for determining whether labour induction will be successful (Tan et al., 2006).
In particular, cervical length as determined by transvaginal ultrasonography is meaningfully associated with premature labor pain, regardless of singleton/ twin pregnancy and the cervical length as determined by this method is routinely implemented to assess the cervical maturity of fully pregnant women (Chung et al., 2015).
The study's objective is to evaluate several cervical and lower uterine segment sonographic markers in order to predict labour induction and vaginal delivery.
Patients and Methods:
After ethical committee approval and informed consent from the patients, this prospective cohort study was performed on total 105 women who were recruited from those attending labor room for induction of labor and willing to participate in the study to investigate the value of the various cervical and lower uterine segment sonographic parameters to predict induction of labor and vaginal delivery at Ain Shams University Maternity Hospital labor room.
Study population:
105 Pregnant women were admitted for induction of labor after cervical and lower uterine segment sonographic assessment.
These included patients aged 20-35 years, pregnant women with a living singleton pregnancy, patients who had no contractions on admission, vertex presentation, gestational age between 37 and 42 weeks and intact membranes at time induction of labor.
While patients with history of previous caesarean delivery, rupture uterus or uterine surgery (due to risk of rupture uterus), Antepartum hemorrhage (due to need of emergency delivery), abnormal fetal lie or presentation (not fit for induction of labor), Category II, III non-stress test (due to need of emergency delivery), Pelvic bony deformity (not fit for induction of labor), Fetal growth restriction or macrosomia (high risk of fetal distress or obstructed labor), Active genital Herpes Simplex (not fit for vaginal labor) and patients who refuse to participate in our study were excluded from the study.
Study procedure:
The Ultrasound study was done by senior staff trained on such procedure
All patients underwent the following:
Informed consent was obtained from all the participants in this study and all participants were subjected to a detailed clinical assessment, including: a detailed history, general, abdominal and pelvic examinations.
Digital vaginal examination was performed to assess cervical consistency, effacement; dilatation, position and station of the presenting part to calculate the BS using the Burnett modification (Burnett, 1966). The results of Manipal score were not available to the assessor of the Bishop Score.
2D obstetric ultrasound and transvaginal ultrasound (TVS) was done after asking the patient to empty the bladder. A MEDISON X6 transvaginal probe (frequency 4–9 MHz 2D) was gently placed in the vagina just below the cervix to avoid undue pressure.
A sagittal view of the cervix was obtained and the image was enlarged by zooming until the cervix occupied at least two-thirds of the image and assessment of the following parameters was done to obtain the Manipal cervical score (Bajpai et al., 2015) (a) Cervical length was measured by placing calipers on the internal OS and external cervical OS, (b) the presence or absence of funneling and if present its width and length at internal OS were measured, (c) the distance between presenting part to external OS, (d) the position of the cervix and (e) Lower uterine segment thickness.
IOL was performed according to the standard protocol of Ain Shams University Maternity Hospital: For the women with a favorable cervix (Bishop Score ≥8), an induction was initiated by amniotomy accompanied by oxytocin infusion (low dose regimen starting with 1 mU/min, increased by 1–2 mU at 30 min intervals (We SQ et al., 2010). For the women with a Bishop Score ˂ 8; IOL was performed by dinoprostone 3 mg vaginal tablet into the posterior vaginal fornix. The cervical dilatation and presence of uterine contractions were reassessed after six hours for the need of another dose of dinoprostone (Maximum of two doses). An amniotomy was performed when the cervix was ≥ 3 cm dilated, and the presenting part was low (‘0’station), and oxytocin drip was started after 6 h of dinoprostone.
Observing the progress of labor was done. The time elapsed until the active phase of labor, the time until delivery and the mode of delivery were recorded.
A failed induction was considered when there was a failure to get regular (at least three minutes apart) contractions and documented cervical change with oxytocin administration at 24 h after artificial rupture of membranes (Spong et al., 2012).
First-stage arrest was defined if no change in cervical dilatation for 4 h despite the presence of adequate uterine contractions or for 6 h if no adequate contractions after reaching the active phase of the first stage of labor (the cervix is 6 cm dilated or more with membrane rupture) (Spong et al., 2012).
Second-stage arrest was documented if failure of the descent or rotation for ≤4 h in nulliparous with an epidural analgesia, or 3 h if epidural analgesia was not used and ≤3 h in multiparous women with an epidural analgesia, or ≤ 2 h without an epidural analgesia (Spong et al., 2012).
Ethical Considerations:
The study was presented for approval from the ethical committee of the department of Obstetrics and Gynecology, faculty of medicine, Ain Shams University. Informed consent after explaining the study purpose and methods to the subjects. Data presentation was not by the patient’s name but by diagnosis.
Statistical analysis:
The collected data was coded, tabulated, and statistically analyzed using IBM SPSS statistics (Statistical Package for Social Sciences) software version 22.0, IBM Corp., Chicago, USA, 2013 and Microsoft Office Excel 2007. Descriptive statistics were done for quantitative data as minimum& maximum of the range as well as mean±SD (Standard deviation) for quantitative normally distributed data, while it was done for qualitative data as number and percentage. Inferential analyses were done for quantitative variables using Shapiro-Wilk test for normality testing, independent t-test in cases of two independent groups with normally distributed data. In qualitative data, inferential analyses of independent variables were done using the Chi square test for differences between proportions and Fisher’s exact test for variables with small expected numbers. The level of significance was taken at P value < 0>
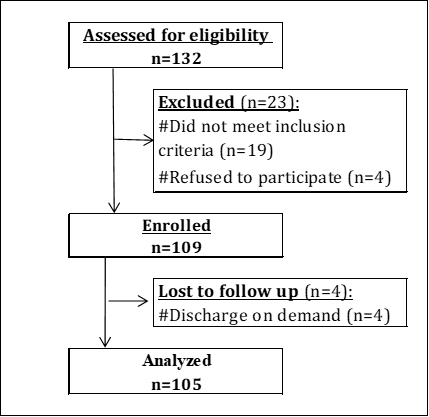
Figure 1: Flow chart of the studied cases.
| Characteristics | Mean±SD | Range |
| Age (years) | 27.4±5.1 | 18.0–37.0 |
| Gestational age (weeks) | 38.9±1.3 | 37.0–42.0 |
| Median (1st−3rd IQ) | Range | |
| Parity | 2.0 (1.0−3.0) | 0.0–6.0 |
Table 1: Demographic characteristics of the studied cases.

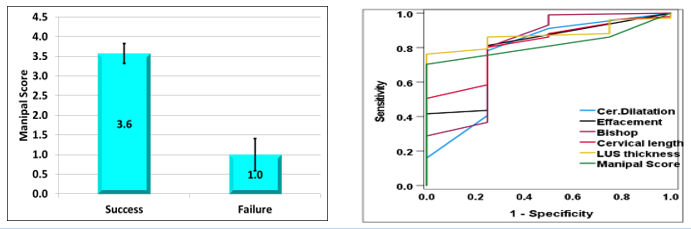
| Figure 4: Comparison according to induction fate regarding Manipal Score | Figure 5: ROC curve for cervical measures in predicting successful induction |

| Figure 6: Comparison according to mode of delivery regarding Bishop Score | Figure 7: Comparison according to mode of delivery regarding LUS thickness |

Figure 8: Comparison according to mode of delivery regarding Manipal Score Figure 9: Correlation between Times until delivery and cervical dilatation among successful induction cases
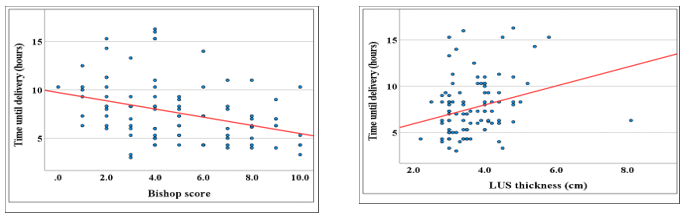
Figure 10: Correlation between Times until delivery and Bishop Score among successful induction cases, Figure 11: Correlation between Times until delivery and LUS thickness among successful induction cases
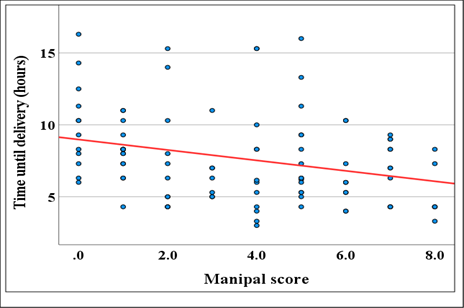
Figure 12: Correlation between Times until delivery and Manipal Score among successful induction cases
The demographics of the patients in the current study are quite comparable. This rule out the chance of any confounding factors influencing the study's findings and interpretation.
Our study showed that induction was successful in the majority of cases (96.2%). Mean± SD of Time until active phase and delivery was 4.1±2.7 and 7.6±3.1 hours, respectively. Normal vaginal delivery was the most frequent mode in the majority of cases (93.3%).
In agreement with our study, (Gonen et al., 1998) showed that induction was successful in the majority of cases.
Our study illustrated that cases with successful induction statistically had significant higher Effacement and Bishop Score.
(Gonen et al., 1998) found that successful induction and labour duration were highly correlated with the bishop score, which is consistent with our findings.
Our study demonstrated that cases with successful induction statistically had significant lower cervical length (P = 0.025) and LUS thickness (P = 0.034) as well as higher Manipal score (P =0.001). It showed that 98 patients had successful induction. 49 cases (48.5 %) had cervical funneling. The mean ± SD of cervical length was 3 ± 0.7 mm in the successful group vs 3.8± 0.6 mm in the failure group. The mean ± SD of thickness of LUS was 3.7 ± 0.8 mm in the successful group vs 4.6 ±0.4 mm in the failure group. Also, the mean ± SD of Manipal score was 3.6 ± 2.5 in the successful group vs 1 ± 0.5 in the failure group.
Similarly, (Hamza et al., 2021) showed that the median CL was 29.9 mm (0–54 mm). 16 patients (11.9 %) had cervical funneling. The median thickness of the LUS was 4 mm (1.8–9 mm). The median strain value of the LUS was 0.55 (0.01–2.03).
Additionally, (Gonen et al., 1998) showed a substantial relationship between the cervical length and both the success of induction and the length of labour. With a range of 13–52 mm, the mean cervical length determined by transvaginal ultrasound was 30 mm (95% confidence interval (CI) 28–33 mm).
Our study showed that Bishop Score (P = 0.045), cervical length (P = 0.034), LUS thickness (P = 0.012) and Manipal score (P = 0.031) had a significant diagnostic performance in predicting successful induction, highest in LUS thickness. LUS thickness ≤ 4.2 cm had the best diagnostic characteristics, except sensitivity which was highest in Bishop Score ≥ 3mm.
Similarly, (Gonen et al., 1998) showed that the threshold of cervical length and Bishop Score that was found to be the best predictor of successful induction were 27 mm and >5, respectively
In agreement with our results, (Roman et al., 2004) showed that the Bishop Score cut-off of 4 had the greatest sensitivity (87.5%) and specificity (45.5%) in predicting failure of induced labor, and this value represents the furthest ROC-curve point from the non-diagnostic line. However, its likelihood ratio is only 1.58 which suggests that the bishop score has a poor discriminatory value for induction failure. Statistical comparison of Bishop Score and cervical length measurement showed that the two ROC curves were not significantly different.
However, (Gonen et al., 1998) prospectively evaluated 86 pregnant women and found that only the Bishop Score and parity were independent predictors of vaginal delivery in induced labor, despite a significant association between ultrasound cervical length and successful induction.
(Ware and Raynor, 2000) showed that both ultrasound cervical length and the Bishop score showed a correlation with vaginal delivery, but cervical length was not an independent predictor. It is difficult to draw definitive conclusions from these studies because of the different inclusion criteria, Bishop Score ranges and induction agents used.
There were few systematic reviews on the role of transvaginal sonography in pre-induction assessment of cervix. (Crane, 2006) reviewed the factors involved in the prediction of successful induction of labour. They concluded that increasing parity and age, lower weight, height and BMI and higher gestational age all were associated with successful induction of labour. They also noted that state of ripening correlated with successful induction and Bishop Score is better in assessing cervical favorability. Even though they acknowledged the usefulness of sonographic cervical assessment in prediction of labour induction, they stated that the superiority of sonographic cervical assessment had yet to be identified.
On the other hand, (Hendrix et al., 1998) did not find that the bishop score was a significant predictive marker for failed induction in 365 women with Bishop Score values between 0 and 13. The evaluation of the bishop score 6 h after the start of induction is also a parameter widely used in current obstetric practice to predict successful labor induction, but the multiple regression model showed that its values are not independent from the initial Bishop Score values.
Significant correlations of digital cervical length and dilatation with successful vaginal delivery have also been reported by (Paterson-Brown et al., 1991) in 50 women undergoing labor induction.
Our study reported that no statistically significant differences according to mode of delivery regarding demographic characteristics. Cases with NVD statistically had non-significant higher Bishop Score. Cases with NVD statistically had significant lower LUS thickness as well as higher Manipal score with no significant difference between AVD and CS.
In disagreement with our results, (Wafa et al., 2018) showed that there were highly statistically significant relations (HS) detected between mode of delivery and cervical length, bishop score and posterior cervical angle as p value (0.001). This may be attributed to the larger number of patients with different demographic characteristics than the patients included in our study. In addition to the higher Bishop score in the patients studied by them (mean bishop score was 7.20 ± 1.80).
Our study showed that times until active phase and delivery among successful induction cases statistically had significant positive correlations with Cervical length and LUS thickness as well as significant negative correlations with Age, Parity, Cervical dilatation, Effacement, Bishop Score and Manipal Score.
Similarly, in 2018 Wafa et al showed highly significant positive correlation detected between induction time and cervical length as p value (0.001) and (r = 0.706) and highly significant negative correlation between induction time and bishop score and posterior cervical angle.
In agreement with our results, (Hamza et al., 2021) showed that CL correlated with the time interval for the onset of labor and rupture of membranes. The functional CL was 25.3 (0–51.5) mm in cases with delivery within 24 hours. In patients who did not deliver within 24 hours, the functional cervical length was 32.2 (7.6–52) mm. Logistic regression revealed a statistically significant impact of CL on delivery within 24 hours (p-value: 0.0012). In the case of cervical funneling, 75.0 % of births were within 24 hours compared to 41.2 % not within 24 hours (p = 0.0150).
Limitation:
Despite the large number of trial participants, each of the 8 different IOL indications has a unique set of causes and patho-mechanics.
The sample size will be less if each IOL indication is examined separately, which will diminish the study's statistical power.
Therefore, to prevent subgroup bias in future trials, it is advised that each indication be examined independently.
Conclusion:
Our research allowed us to show evidence that the internal OS level of the cervical structure underwent shortening through funneling. These structural changes could be what make for an effective induction of labour.
Pre-induction cervical length and LUS thickness measurements in women undergoing labour induction give considerable independent prediction of the induction process
Bishop scores were exceeded by sonographic factors in terms of predicting the success of induction.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
