
Case Report | DOI: https://doi.org/10.31579/2690-1897/131
1Head of Department of Neurosurgery Bejaia Hospital, Bejaia, Algeria.
2 Neurosurgery Department, Mustapha Pacha University Hospital, Algiera.
*Corresponding Author: Bekralas H. 1Head of Department of Neurosurgery Bejaia Hospital, Bejaia, Algeria
Citation: Bekralas H and Habchi N. (2022). Cerebrospinal Fluid Ascitis: Late Complication of A Ventriculo-Peritoneal Bypass, 5(7) DOI: 10.31579/2690-1897/131
Copyright: © 2022 Bekralas H. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 October 2022 | Accepted: 29 October 2022 | Published: 09 December 2022
Keywords: LCS ascites; ventriculoperitoneal bypass; ventriculo-atrial bypass
Cerebrospinal fluid (CSF) ascites is a rare complication of ventriculoperitoneal shunt (PVD). The etiological factors and especially the mechanisms underlying this complication remain difficult to explain. We report the case of a voluminous CSF ascites complicating a DVP, 15 years later. This is a 16-year-old patient, valved at the age of one year, admitted for major abdominal distension. The abdominal scanner shows a large free fluid collection in the peritoneal cavity. The puncture of this ascites and above all the conversion of the DVP into a ventriculo-atrial bypass allowed the collection to dry up. The various hypotheses mentioned in the literature struggle to explain the occurrence of ascites in this patient. This ascites seems to stem from a progressive failure of the mechanisms of peritoneal resorption over time and this apart from any primary peritoneal pathology.
CSF diversion into the peritoneal cavity was performed by Kausch for the first time in 1908 [1]; Since then, the ventriculo-peritoneal (VPD) shunt has been the most widely used technique for the treatment of hydrocephalus. It offers a high success rate if we refer to the longevity of the patients [2]. Abdominal complications related to this technique are frequent, CSF ascites is rather rare and often appears late [3]. We report a voluminous CSF ascites that occurred 15 years after a ventriculoperitoneal shunt. This is the first case of LCS ascites reported after such a long period. The mechanisms and causes that can explain this complication are discussed through a review of the literature.
This is a 16-year-old patient treated in our department at the age of one year for hydrocephalus. The clinical examination at the age of one year showed left hemiparesis and convergent strabismus, while the cranial circumference was normal.The cranio-encephalic scanner revealed right univentricular hydrocephalus (Fig1), a ventriculoperitoneal valve of medium pressure was put in place with simple consequences.
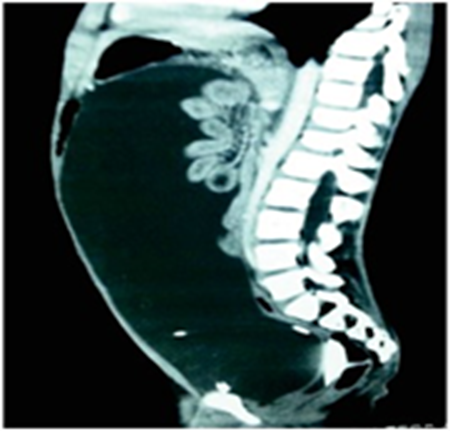
Figure1. Right univentricular hydrocephalus
The patient was admitted again 10 months later for the management of a dysfunction of the valve, the revision of which found an obstruction of the distal drain. 15 years later, the patient presented with intense abdominal pain with cessation of matter and gas. The general condition is altered. Examination of the abdomen reveals significant abdominal distension hampering thoracic expansion and thus preventing any supine position, there is no palpable mass or sign of peritoneal irritation. The percussion shows a dullness extended to the whole of the abdomen, maximum on the flanks; this symptomatology is in favor of an intraperitoneal fluid effusion. The abdominal CT shows a large free fluid collection in the peritoneal cavity causing major visceral compression (Fig.2).
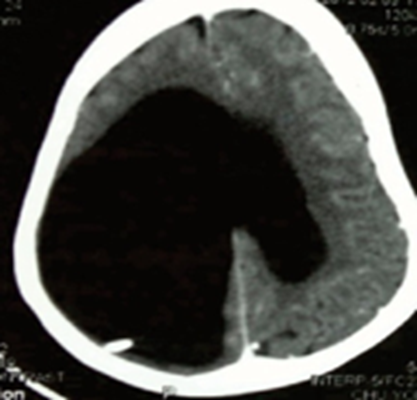
Figure 2: Abdominal CT scan in sagittal reconstruction showing CSF ascites. Note the presence of the distal drain with in the collection
The biological assessment shows a hemoglobin level at 10.5 g / dl and a number of white blood cells at 9000 elements / mm3, a natremia 144 mmol / l, a potassium level at 4.8 mmol / l, a chloremia at 110 mmol /l, a calcemia at 97.8 mg/l and a Magnesemia at 17.8 mg/l. The transaminase level is normal and the esophagogastroduodenal fibroscopy did not show any esophageal varices, thus eliminating portal hypertension. Cranio-encephalic CT shows right univentricular hydrocephalus. Faced with these signs, a disorder of peritoneal resorption of CSF is evoked and the liquid collection is drained gradually at low flow.Macroscopic examination finds a citrine liquid, transudative (rivalta negative), no germs are found on bacteriological examination. A ventriculo-atrial bypass is performed, the ascites has dried up completely
This is a rare case of CSF ascites complicating ventriculoperitoneal shunting. This complication does not seem to pose a problem of clinical description and therapeutic management. On the other hand, the mechanisms leading to the defect of resorption of the CSF by the peritoneum are still the subject of discussion. LCS ascites seems to be due to multifactorial causes and mechanisms [4]. Ray [5] reported the occurrence of LCS ascites in a case of choroid plexus papilloma incriminating LCS hypersecretion as the mechanism behind this ascites. This hypothesis did not seem to be unanimous since all CSF shunts related to choroid plexus papillomas were not complicated by ascites.Some authors [6] mentioned the elevation of the protein level in the CSF as a possible cause of the occurrence of ascites, while for others peritoneal infection by blocking lymphatic drainage was another cause [7]. Dean et al [8] reported ascites linked to immuno-allergic phenomena in response to an antigen-antibody reaction following vaccination against diphtheria and tetanus. The hypotheses are therefore multiple without any of them being able to explain the mechanism allowing the occurrence of ascites. Abdominal surgery is a contributing factor to the occurrence of CSF ascites found in many patients; if for Michiko et al [9], the ascites would occur less than 2 years after the surgery, this hypothesis cannot be accepted in the case of this patient, in whom the ascites occurred 15 years after the diversion and 14 years after revision of the peritoneal catheter.Peritoneal biopsy found eosinophilic infiltration reflecting a foreign body reaction, however, no peritoneal pathology was found to explain the lack of resorption in most patients [10].On reading the data in the literature, none of the previously mentioned hypotheses can explain the occurrence of ascites in the case presented. It is therefore a progressive failure of the mechanisms of peritoneal resorption apart from any primary peritoneal pathology and whose only contributing factor seems to be the high age of the diversion. A major axis of discussion remains, in our opinion, the discovery of the precise mechanisms according to which this progressive failure of peritoneal resorption would occur over time. This case demonstrates that patients who had a ventriculoperitoneal shunt early in childhood remain subjects at major risk of occurrence of CSF ascites in relation to this progressive failure of the resorption mechanisms.
LCS ascites is a rare complication of ventriculoperitoneal shunting. This is the first reported case of CSF ascites occurring 15 years after bypass. Many hypotheses try in vain to explain the occurrence of this complication. The progressive failure of peritoneal resorption mechanisms over time seems to be the cause of this ascites. The possibility of occurrence of this failure with the advanced age of the DVP requires increased monitoring of patients derived very early in childhood.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
