
Case Report | DOI: https://doi.org/10.31579/2641-0419/502
1Faculty of medicine and biomedical sciences, University of Yaoundé, Yaoundé, Cameroon.
2Department of internal medicine, Garoua general hospital, Garoua, Cameroon.
3Department of internal medicine, Yaoundé university teaching hospital, Yaoundé, Cameroon.
4Faculty of medicine and pharmaceutical sciences, University of Douala, Douala, Cameroon.
5Department of internal medicine, Douala general hospital, Douala, Cameroon.
*Corresponding Author: Hamadou Ba, Senior lecturer at the faculty of medicine and biomedical sciences; General Manger of the Garoua general hospital, Head of the Internal Medicine.
Citation: Hamadou Ba, Nganou-G C-Nadège, Hassana Samir, Hadja Inna Astasselbe, Kamdem Félicité, (2025), Cerebral Venous thrombosis in SS homozygous Sickle Cell Disease Associated with Hypothyroidism: a Case Report, J Clinical Cardiology and Cardiovascular Interventions, 8(12); DOI:10.31579/2641-0419/502
Copyright: © 2025, Hamadou Ba. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 30 June 2025 | Accepted: 04 August 2025 | Published: 14 August 2025
Keywords: cerebral venous thrombosis; homozygous; sickle cell disease; hypothyroidism
Cerebral venous thrombosis (CVT) is a rare form of stroke that affects the venous system. It’s a multifactorial condition, which may be triggered by hemoglobinopathies such as sickle cell disease (SCD). We report the case of a SCD patient, admitted in the Internal Medicine department for progressively worsening headaches associated with generalized seizures. The diagnosis of superior sagittal sinus thrombosis associated with hypothyroidism was made. The clinical outcome was favorable with anticoagulation. This case highlights the importance for clinician to not overlook SCD, and hypothyroidism as relevant etiological factors of CVT.
Cerebral venous thrombosis (CVT) is a form of stroke affecting the venous system, particularly dural venous sinuses. It represents 0.5 to 1% of all stroke cases and mainly affects young adults, especially women with prothrombotic conditions [1]. Many conditions may contribute to the occurrence of CVT, such as clotting and endocrine disorders, and hemoglobinopathies like sickle cell disease (SCD)[2,3]. The clinical presentation of CVT is polymorphic, depending on the location and extension of the thrombosis. The most frequent symptoms are headaches (80 to 90% of cases), associated with visual disturbances, seizures, motor or sensitive deficits, altered mental status and/or meningeal syndrome [4]. Some recent studies suggest the implication of hypothyroidism and SCD, in the development of clotting disorders as well as thromboembolic diseases [5,6]. We report a case of CVT in a SCD patient who also had hypothyroidism, illustrating complex etiopathological mechanisms.
A 50 years old woman with SS homozygous SCD diagnosed in her childhood, but lost to follow-up, was admitted in the internal medicine department of the Garoua general hospital. She presented with worsening headaches, associated with a generalized tonic-clonic seizure which occurred one day before admission. The history revealed that the patient had received a blood transfusion for anemia, five days earlier. Physical examination showed left facial palsy and a left pyramidal syndrome with 4/5 muscle power. A head CT-scan was done showing diffuse cortical atrophy. We pushed the investigations further by performing a magnetic resonance angiography which showed a thrombosis of the superior sagittal sinus (figure 1). Laboratory workups showed normocytic normochromic anemia with 8.5 g/dl of hemoglobin. Basic hemostasis tests were normal. HIV and hepatitis B and C serologies were negative. Serum creatinine was 169mg/dl (glomerular filtration rate = 41.31ml/mn/1.73m2) and the natremia was 159mmol/L. Thyroid function tests revealed a hypothyroidism with a TSHus of 1.008 UI/mL, FT4 of 1.61pmol/L and FT3 of 9.881pmol/L. Thrombophilia and immunological investigations were not done because of timing and logistical constraints. The patient was treated with low molecular weight heparin switched with acenocoumarol (target INR 2-3), carbamazepine 200mg bid, nefopam 10mg tid, levothyroxine 25µg od, and hydration with crystalloids (1500mL/day). The outcome was favorable with amendment of headaches, seizures, and normalization of kidney function and natremia.
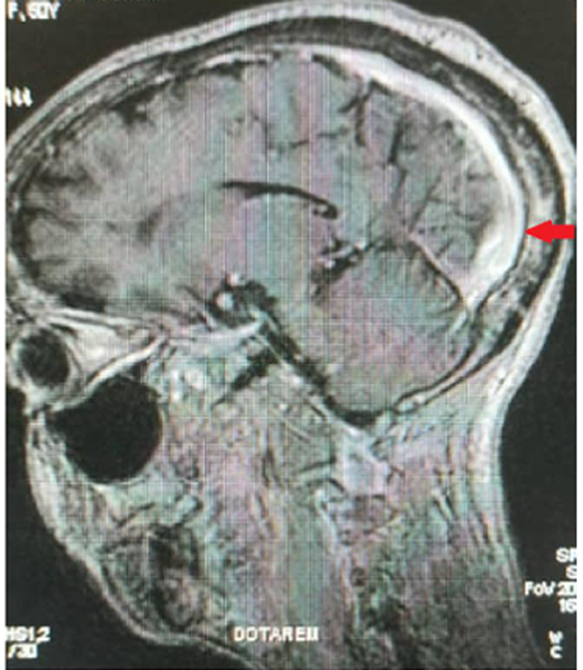
Figure 1: Cerebral magnetic resonance angiography showing the thrombosis of the superior sagittal sinus (red arrow)
The clinical spectrum of CVT is large. The classic presentation includes signs of raised intracranial pressure, focal neurologic deficits and/or seizures. All these signs were present in the case of our patient. CVT is a multifactorial disease, which can result from as many risk factors as hereditary thrombophilia, oral contraceptives, pregnancy and post-partum period [4,7]. Some studies have also showed the involvement of SCD in clotting activation. In fact, SCD patient exhibit low plasmatic level of C and S proteins, while there is an increase of tissue factor expression and thrombin formation [6]. These patients also present moderate thrombocytosis due to functional asplenia, and increased platelet aggregation [6]. Other evidence reports increased adhesion of sickle red blood cells to the endothelium [8]. Recent studies have reported cases of hypothyroidism in patients affected by CVT [9,10]. Hypothyroidism may promote a hypercoagulable state by decreasing fibrinolysis through high level of alpha 2-antiplasmin and plasminogen activator inhibitor-1. The rare association of SCD and hypothyroidism inexorably leaded to the pathogenesis of CVT in this patient.
Cerebral venous thrombosis is a rare disease, with multiple causes, among which sickle cell disease and hypothyroidism should not be overlooked. They play an important role in alteration of the clotting cascade. Consequently, these etiologies should be investigated in all cases of CVT.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
