
Case Ropert | DOI: https://doi.org/10.31579/2639-4162/017
*Corresponding Author: Study undertaken in the Department of Anesthesia-Resuscitation, Hospital, Morocco
Citation: Lazraq Mohamed, Bensaid abdelhak, Miloudi Youssef, and Elharrar najib. Cerebral Empyema Complicating a Dental Abscess. j. General medicine and clinical practice. DoI: 10.31579/2639-4162/017
Copyright: © 2019 Lazraq Mohamed. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 March 2019 | Accepted: 15 April 2019 | Published: 24 April 2019
Keywords: dental abscess; cellulitis; cerebral empyema
Cervico-facial cellulitis can cause serious complications including neuro-meningeal infections. Among these neuro-meningeal infections are intracranial empyemas, which are rarer than brain abscesses.
We report the case of a young patient of 25 years, immunocompetent, having presented a cerebral empyema secondary to diffuse cervicofacial cellulitis of dental origin. The diagnosis was suspected in the presence of cervicofacial cellulitis, febrile meningeal syndrome and consciousness disorder, confirmation was reported by brain MRI. The evolution was favorable after the recourse to the surgical treatment.
Cervico-facial cellulitis is a severe infection of the subcutaneous cellular tissue of the face and is most often of dental or peridental origin. It can be at the origin of serious complications including neuromeningeal infections [1].
Although it is a rare complication, especially in young adults who are incompetent [7-8], it remains serious and may be life-threatening.
Cerebral abscesses are preferentially located in the parietal or frontal lobe [2, 3]. Intracranial empyemas are rarer than cerebral abscesses, account for 25-31% of intracranial suppurations [4], 75% being subdural [5,6].
We report in this paper the case of a patient who developed a subdural empyema secondary to diffuse cellulitis of dental origin in a 25-year-old boy.
Observation:
This is a 25-year-old patient with no pathological history, admitted to otorhinolaryngological emergencies for cervicofacial cellulitis. The symptomatology was two weeks earlier by the appearance of a dental abscess initially treated with a nonsteroidal anti-inflammatory drug and a spiramycin antibiotherapy. The evolution was marked by the appearance of a red and hot swelling in the cervicofacial and temporal region.
At admission, the patient was confused, Glasgow score at 14/15, without deficit, symmetrical and reactive pupils, hemodynamically stable and respiratory, feverish at 40 ° C, the clinical examination objectified a neck stiffness.
The lumbar puncture was in favor of bacterial meningitis. The patient underwent surgical drainage of cellulite with tri-antibiotherapy based on ceftriaxon (meningeal dose), metronidazole and moxifloxacin. It should be noted that the immunological assessment of the patient was normal and the HIV serologies were negative. Bacteriological examination of pus revealed a multisensitive streptococcus SPP.
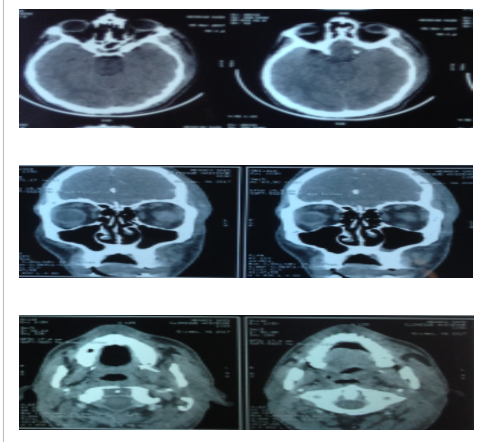
On day 2 of hospitalization, the patient presented generalized tonic-clonic convulsions, which necessitated the realization of a cerebral MRI showing left subdural temporo-parietal empyema with diffuse enhancing meningeal (image 2).

One week later, the patient experienced an alteration of his neurological status with control MRI worsening the left temporoparietal subdural empyema (image 3).

Surgical drainage of the empyema was performed with a favorable evolution. The bacteriological examination of pus also objectified the same germ which is streptococcus spp multi-sensitive.
Discussion:
Serious cellulitis is a serious infectious emergency especially in developing countries [9].
The mortality rate is high when effective management is not undertaken [9,10]. Inadequacy of primary treatment (inadequate antibiotic therapy and use of nonsteroidal anti-inflammatory drugs for analgesic purposes) is used as an adverse factor for the occurrence of serious infectious complications.
The diffuse cellulitis complications are numerous and serious (pleuropulmonary infection, mediastinal, thrombophlebitis, cerebral abscess ...). The prevalence of a dental infection for cerebral infections ranges from 2.7% to 6.5% [11].
The diffusion of the oral germs at the cerebral level can be made by contiguity within the framework of an acute infection or then by hematogenous way with the chronic foci [10]. The microbial flora found in cerebral abscesses of dental origin is polymorphic. In 70% of cases, we find streptococci [12], which is the case in our patient.
Cerebral abscess is thought to be the consequence of hematogenous dissemination of dental infection via the facial and ophthalmic veins where the germs enter the skull through the cavernous sinus [13,14,15].
In fact, the known dental sources of cerebral infections include tooth abscess, cellulitis, periodontitis, extractions, canal treatments, and the placement of orthodontic appliances [16-17].
Bacteriologically, the most frequently responsible germs are streptococci and particularly those of the intermedius group, including Streptococcus anginosus [18].
Brain empyemas may be polymicrobial (40% of cases), especially if the germs originate from the oropharynx (association of streptococci and anaerobes). Other bacteria can also be found, depending on the portal of entry: enterobacteria, pyocyanic, staphylococcus aureus [18].
However, in each case where a dental origin is suspected, the eradication of infectious foci must be rigorous and must leave no room for doubt.
Regarding the cerebral infection, the classical treatment, included an urgent surgical evacuation supervised by an antibiotherapy, with a systematic size of a large shutter allowing a washing and a sufficient drainage of the empyema and the purulent cavities which are often compartmentalized by distance [19, 20, 21].
Currently, the latest generation antibiotics allow medical treatment without surgery, in the same way as the entryway treatment, and for up to 3 months [22, 23].
Antibiotic therapy is chosen with reference to isolated germs in the empyema and in the entryway. The surgical procedure is however necessary if the volume of the empyema determines signs of intracranial hypertension or if it increases in volume. It can be limited to the holes of trephine opposite the collection, or a large craniotomy allowing the complete evacuation of empyema, primary infectious foci and possibly verification of the absence of other localizations at different stages of the brain [20,24]. After collection evacuation, a drainage installation for a few days was often recommended by the authors [20,25].
Conclusion:
Indeed, the cerebral infectious localizations are certainly rare but providers of an important morbi-mortality, even if in our case the evolution was completely satisfactory. Intracranial suppurations constitute a medico-surgical emergency and their optimal management is a multidisciplinary collaboration (reanimateur, neurosurgeon, otolaryngologist, bacteriologist, radiologist...). otorhinolaryngological pathology remains the main entry point of these affections.
The diagnosis is based on the clinic and the radiology. The scanner is the first-line examination, it allows to make the diagnosis, to guide the therapeutic behavior and to follow the evolution. MRI sometimes performs better than CT. Sterile cultures have become increasingly common due to the early prescription of antibiotics. The prevention of these dreadful complications is based essentially on the eradication of infectious otorhinolaryngological and especially dental foci.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
