
Case Report | DOI: https://doi.org/10.31579/2692-9406/130
1 Central Radiology Institute, Kepler University Hospital, Medical Faculty of the Johannes Kepler University, Linz, Austria.
2 Institute of Neuroradiology, Kepler University Hospital, Medical Faculty of the Johannes Kepler University, Linz, Austria.
3 Medical Faculty of the Friedrich-Alexander-University of Erlangen-Nürnberg, Erlangen, Germany.
*Corresponding Author: Michael Hofko, Central Radiology Institute, Kepler University Hospital, Medical Faculty of the Johannes Kepler University, Linz, Austria.
Citation: Michael Hofko, Michael Sonnberger, Franz A. Fellner, (2022), Cerebral Dural Arterio-Venous Fistula – Part II: Endovascular Therapy with Transarterial Embolization using Liquid Embolization Material. Biomedical Research and Clinical Reviews, 7(4); DOI:10.31579/2692-9406/130.
Copyright: © 2022, Michael Hofko, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 August 2022 | Accepted: 29 September 2022 | Published: 26 December 2022
Keywords: cerebral dural arterio-venous fistula; digital subtraction angiography; endovascular; interventional radiology; embolization; onyx; transfemoral angiography; computer tomography (CT)
Case report of a 60 years old male patient with recent diagnosis of an occipital dural arteriovenous fistula classified CognardTyp IV, treated by transfemoral cerebral angiography and embolization with liquid embolization material (Onyx).
Dural arteriovenous fistula (DAVF) is a type of AVM in which there is a communication between dural arteries and cerebral venous sinuses. These lesions constitute 10–15% of all cerebral AVMs and most of them seemed to be acquired, only some are congenital. There is a female to male ratio of 2:1 and most of them are diagnosed in the fifth and sixth decade. The distinguishing feature between DAVF and cerebral AVM is the fact that there is no parenchymal nidus and there is a dural arterial supply [1].
We demonstrate a case of a 60-year-old man with recent diagnosis of an occipital dural arteriovenous fistula classified Cognard Typ IV, treated by transfemoral cerebral angiography and embolization with liquid embolization material (Onyx - composed of a mixture of ethylene–vinyl alcohol copolymer suspended in the solvent dimethyl sulfoxide (DMSO) – Tantalum is added for radiopacity).
We present a case of a 60-year old male patient with recent diagnosis of an occipital dural arteriovenous fistula classified Cognard Typ IV, treated by transfemoral cerebral angiography and embolization with liquid embolization material (Onyx).
The therapeutic angiography was performed in intubation anesthesia, our interventional neuro radiologist took the common femoral artery as an arterial access supported by a 6-F-vascular lock, a 6-F-guiding catheter was positioned in the left maxillary artery (Figure 1), furthermore a distal access catheter was placed at the branchpoint of the middle meningeal artery(Figure 2). Using this guiding catheter a microcatheter was positioned at the origin of the fistula.
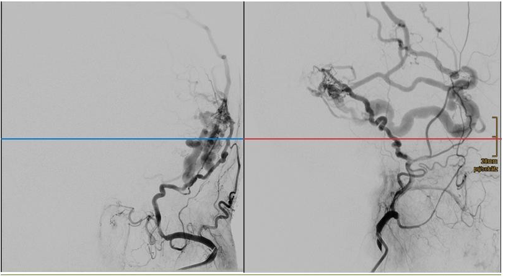
Figure 1: showing the catheter in the left maxillary artery a) ap position; b) side view
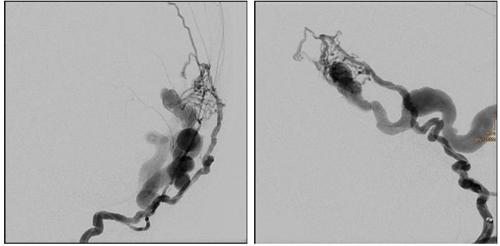
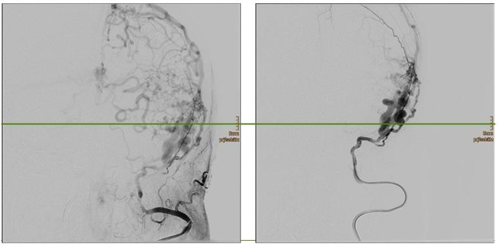
Figure 2: a/b showing the distal accesssecond catheter (ACCESS®) at the branch point of the middle meniongeal artery
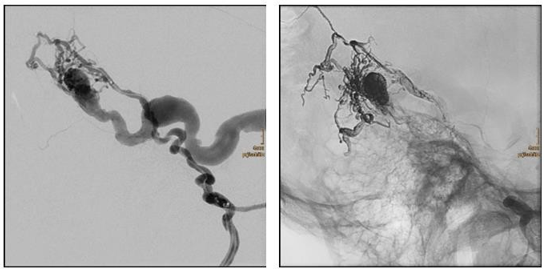
Figure 3: a positioning of the microcatheter in front of the arterial feeders; b digital subtraction angiography showing the veins onyx cast with complete obliteration of the fistula.
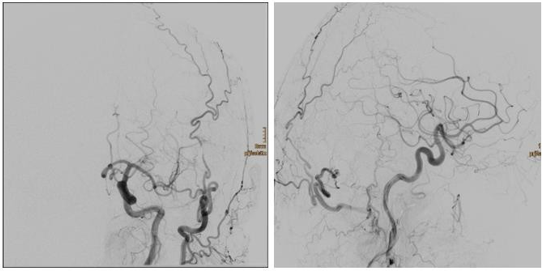
Figure 4: a/b (a ap-view;b side view) digital subtraction angiography of the left common carotid artery showing noresidual fistula.
Our used technique of trans arterial embolization is ideally used for high- grade DAVFs, such as those with direct cortical venous drainage, or in situations in which venous access is limited. There is a list of the advantages of the trans arterial embolization technique:
(1) there is the possibility to occlude the arteriovenous fistula transition through a trans arterial approach, decreasing the possibility of flow diversion into an alternate venous pathway.
(2) using this technique there is no limitation by venous access(e.g., stenotic or thrombosed venous sinuses).
(3) after the arterial pathway there is no higher risk of venous complications.
(4) trans venous embolization can be followed by secondary site as de novo DAVFs resulting of venous hypertension.
(5) by this technique specific complications to trans venous routes can be avoided (e.g., abducens nerve palsy from catheterization of the superior petrosal sinus) [1].
Using as super selective microcatheter angiography, three-dimensional, rotational angiography and a form of high-resolution flat-panel computed tomography (CT) known as “DynaCT” are recommended in defining the arterial and venous anatomy of a DAVF both before and after embolization. To prevent premature polymerization and contamination of diagnostic catheters and solutions, embolic agents such as Onyx should be handled on a separate able when not in use, furthermore a separate set of gloves should be used prior to handling these agents and at the end of the procedure prior to final diagnostic angiography [1].
Onyx is one possibility of liquid embolization, it is composed of a mixture of ethylene–vinyl alcohol copolymer suspended in the solvent dimethyl sulfoxide (DMSO) – Tantalum is added for radiopacity- and first reports were published in the 1990, this drug is available in Europe since 1999.
Trans arterial embolization technique is recommend in dural arteriovenous fistulas Cognard Typ IIb – V.
Classification of dural arteriovenous fistulas (Cognard):
| I | Normal antegrade flow in to dural sinus |
| II |
|
| III | Direct drainage into cortical veins without venous ectasia |
| IV | Direct drainage into cortical veins with venous ectasia >5 mm and 3x larger than diameter of draining vein |
| V | Drainage to spinal perimedullary veins |
[2] There are some technical advantages by using ONYX:
For planning the intervention the following points should be considered.
After the embolization procedure an immediate cerebral CT scan is recommend, furthermore you should care about pain medication caused by the dural involvement and low-molecular weight heparin should be prescribed for 1 to 4 weeks to avoid venous thrombosis [1].
Disclosure
All co-authors do not report conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
