
Review Article | DOI: https://doi.org/ 10.31579/2639-4162/030
1 Department of Radiology, San Paolo Dental Building, University of Milan, Italy.
2 San Paolo Dental Building, University of Milan, Italy.
3 IRCCS Ca’ Granda Foundation General Hospital University of Milan, Italy. 4Private Dental Practice, Cagliari, Italy.
*Corresponding Author: Cinzia Casu, Private Dental Practice, Cagliari, Italy.
Citation: Caggiula A, Di Loreto M, Pettinicchio M, Vendrame A, Casu C. (2020) Central Giant Cell Granuloma: A Narrative Review Of Radiological Features And Differential Diagnosis. General medicine and Clinical Practice. 3(2) DOI: 10.31579/2639-4162/030
Copyright: ©2020 Cinzia Casu. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 August 2020 | Accepted: 12 September 2020 | Published: 18 September 2020
Keywords: central giant cell granuloma; maxillary bone lesions; radiographic features of maxillary and jaw lesions
The Central Giant Cell Granuloma is an uncommon lesion, accounting less than 7% of all benign jaw lesions. In 1953, Jaffe was the first to describe these lesions as a giant cell reparative granuloma of the jaw bones, and in 1971, thanks to Pindborg and Kramer, it was included in the current nomenclature. The aetiology of CGCG is unknown, there is also a peripheral type that some authors consider the most common in maxillary bones. WHO defines CGCG as an intraosseous lesion consisting of cellular fibrous tissue that contains multiple foci of hemorrhage, aggregations of multinucleated giant cells, and some trabeculae of woven bone. The radiographic appearance of CGCGs is not pathognomonic. CGCGs should be differentiated from other lesions of the jaws such as Brown’s tumour of hyperparathyroidism, fibrous dysplasia, aneurysmal bone cysts, giant cell tumours, fibro-osseous lesions, and other malignancies that arise in the jaw bones. Furthermore, it needs to be differentiated even from some genetic syndromes, such as Cherubism, type 1-neurofibromatosis and Noonan’s syndrome. The aim of this study is to focus on radiographic features of CGCG in order to achieve an appropriate tool for diagnosis.
Central giant cell granuloma is a benign intraosseous lesion first described by Jaffe. It was hypothesized that the lesion is not a true neoplasm but merely the result of a local reparative reaction [1]. The WHO defines CGCG as an intraosseous lesion consisting of cellular fibrous tissue that contains multiple foci of hemorrhage, aggregations of multinucleated giant cells, and some trabeculae of woven bone [2]. In 2004 epidemiological findings of CGCG in a general population were published. In this report an incidence of 1.1 per 106 was found for the whole population. They very rarely affect the mandibular condyle [3].
A study published in 2012 highlights that these lesions were more prevalent in women than in men, at a 1.56:1 proportion. The mean age of the patients was 25.8 ± 15.3 years (range 0-85). The lesions were more prevalent in the mandible in comparison with the maxilla, but there was no clear prevalence concerning the different regions of the jaws [4].
The origin of this lesion type remains unknown; the lesion may be reactive, a developmental anomaly or a benign neoplasm [5, 6, 7]. This lesion usually appears as a painless, slow-growing swelling of the jaw. Sensory disturbance and pain are not common. Displacement of tooth sometimes occurs, leading to malocclusion. An appropriate CGCG differential diagnosis is made taking into consideration the following hypothesis: odontogenic keratocyst, odontogenic myxoma, odontogenic fibroma, ossifying fibroma, adenomatoid odontogenic tumor, ameloblastoma and central arteriovenous hemangioma. Also aneurysmal bone cyst, Cherubism, fibrous dysplasia, giant cell tumor and brown tumor from hyperparathyroidism, in addition to being indistinguishable radiographically from CGCG, contain multinucleated giant cells [8, 9]. Moreover, neurofibromatosis type 1 syndrome and Noonan syndrome can show lesions similar to CGCG [10]. Because of the indistinguishable radiological features and histological pattern of all these lesions, it is necessary to consider all of them in the differential diagnosis.
Chuong et al. were the first to differentiate between aggressive and nonaggressive lesions on the basis of signs, symptoms and histological features. Aggressive lesions are characterized by one or more of the following features: pain, paresthesia, root resorption, rapid growth, cortical perforation, and a high recurrence rate after surgical curettage. Aggressive lesions were also larger in size and histologically demonstrated a larger fractional surface area occupied by giant-cells. Currently, clinical signs and symptoms and radiological features are the main criteria to differentiate nonaggressive (indolent) from aggressive lesions. According to the same studies, the number and volume of giant-cells checked with other components of the lesion might give a sort of prediction on its clinical behavior [11, 12]. In CGCG, 2 major histological features are diagnostic. There is a highly cellular, fibroblastic stroma with plump, spindle-shaped cells with a high mitotic rate; also vascular density is high. These spindle- shaped cells probably are the proliferating tumor cells, considering that they survive in culture after passing wells and immunohistochemically stain positive for the proliferation marker PCNA. The multinucleated giant- cells are prominent throughout the fibroblastic stroma but are not necessarily abundant. They are usually irregularly distributed and are often located most numerously around areas of hemorrhage [13, 14, 15, 16, 17, 18].
It is necessary, nowadays, to consider all the different radiological techniques and rely on a histology laboratory in order to achieve correct diagnosis as soon as possible, which is critical on choosing the best therapy option.
Materials and Methods
This narrative review was performed by searching on the PubMed search engine.
MeSH terms and keywords were “central giant cell granuloma” resulting in 3390 articles. Only articles published after 1980 and articles with full text available were included.
Inclusion criteria were:
At the end, we obtained 982 potentially useful articles. We excluded not relevant articles after abstracts observation.We analyzed 93 articles (Figure 1) and 21 resulted significant.

Results and Discussions
Although the CGCG does not present a high index of incidence, it requires an appropriate diagnostic framework during the clinical activity, through the use of imaging techniques and appropriate conduct of the objective examination. Most patients present themselves at the clinical examination with an asymptomatic swelling at the facial level or at the level of the oral cavity. It is rarely accompanied by paraesthesia [10].
The imaging results essential to the CGCG diagnosis for its identification, description, pre-surgical evaluation, and post-operatory follow up.OPG is at the moment the referential imaging technique, the CBT with the software emulation dedicated to the study of the dental arches, allows an optimal vision of the bone; it provides meaningful informations in order to differentiate the malign lesion and allows to plan an appropriate surgery [8].
The radiographic features of the CGCG are not specific, for that it is possible to find dissimilar descriptions in literature.
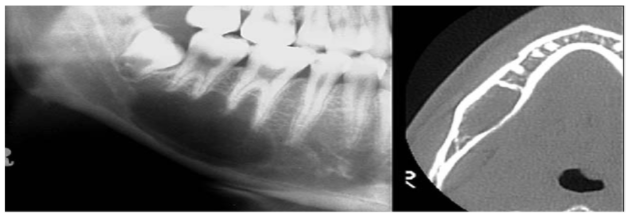
The lesion can present itself as a radiolucent unilocular area or multilocular, to margins well defined or diffused. They described the possibility to resort roots, different degrees of expansion, and the erosion of the cortical bone, which can be appreciative due to the CBT [19, 20].
Radiological characteristics specific to the CGCG
CGCG can present different characteristics. It is a lesion that can vary from small apical osteolysis to a significant destructive lesion that affects the mandible and, with minor frequency, the jaw [10, 21].
It appears as a cyst-like unilocular radiolucent lesion in the majority of the case, or multilocular, with the appearance similar to “soap bubbles” due to the internal presence of septa radiopaque of variable dimensions [10, 22].
The term “multilocular” can, in some instances, be used incorrectly, because of the presence of calcifications within the lithic lesion that can mimic a real and proper multilocular [22]. In the academic literature, it is possible to find lesions cases entirely radiolucent, or radiolucent with variable radiopaque components within the internal radiolucency [23]. The CGCG presents typically well-defined borders to a low index of growth; only in rare cases, they can be diffused [23].
It can cause a dislocation of the dental elements, resorption of the roots and of the inter-radicular bone [9, 23].
The cortical bone usually remains intact but thinned; however, in the academic literature, there are cases of evident cortical resorptions, with the lesion that extends its soft tissues in the surrounding areas [24]. CGCG size can vary from 1 to 7 cm in diameter [22].CBT should be used to determine the greatness, as the orthopantomography (OPG) results inadequate since it tends to underestimate the dimensions [21].
Distinctive characteristics to specific locations
The preferred locations of the CGCG are the maxillary bones, with a higher prevalence within the jaw, in particular in the anterior region [10] [21]. Some authors report several jaw cases; the mandible:maxilla ratio is 3:1 [21].
It generally presents itself as an isolated lesion, the rare cases of multiple and simultaneous are often associated to systematic disorders and hereditary syndromes; it is then less likely that such lesions represent cases of bilateral CGCG [21]. In academic research 5 CGCG cases have been documented at the mandibular condyle level, in the specific case, they result to be with prevalence multilocular or surrounded by a well-defined cortical layer [20, 25]. It highlights that through the use of CT and MRI, it is possible to outline CGCG cases at the neurocranium level. They present themselves in the form of expansive lesions capable of penetrating the soft tissues [24].
The classification of “aggressive” and “not aggressive” CGCG cases
In a few cases, the CGCG can outline some aggressive features in the clinical and radiological analysis. In 1986 Chuong et al. and in 1987 Ficarra et al. suggested a classification between “aggressive” and “non aggressive” CGCGs according to the clinical and radiological characteristics.
The non-aggressive form, the most common, highlights a slow growth associated with more or fewer levels of swelling, painful and paraesthesia. Radiographically, these cases present themselves as unilocular or multilocular radiotransparent distinct areas. It is possible to identify cortical perforations and root resorption, with a lower possibility of recurrence after surgical treatment than the aggressive counterpart. The aggressive form outlines dimensions higher than 5 cm, a rapid growth recurrences after surgical curettage. Also, thinning and/or perforation of the cortical bone, teeth dislocation, and radicular resorption [11, 12].
Kaban et al. modify further the definition; they affirm that in order to classify an aggressive form of CGCG, it is sufficient that it presents dimensions greater than 5 cm and the possibility of recurrences, even when other features are not identified [12]. These cases highlight that aggressive features present themselves more often to pediatric patients [26]. Infantile patients have the cranial bones in the stage of the development and inside the jawbones the process of odontogenesis is still ongoing, with the substitution of deciduous dentition aside the permanent one, these could be etiological factors predisposing to aggressive CGCG cases [27].
It must also be outlined that the radiological diagnosis is challenging to identify in pediatric cases due to the overlapping of the teething elements [27]. The distinction between aggressive and not aggressive CGCG cases is significant because it leads to different therapeutic protocols. Based on these data, the clinical and radiological CGCG characteristics seem to belong to an aggressive benign tumor, rather than granuloma, with some authors suggesting a nomenclature review [28].
Clinical and radiographic differential diagnosis
The radiographic CGCG appearance is not pathognomonic. It can be confused with different sorts of multilocular, expansive and radiolucent lesions of the maxillary. They are distinguishable between the use of imaging techniques [21, 23, 29].
The CGCG differential diagnosis cases are the following: odontogenic keratocyst, odontogenic myxoma, odontogenic fibroma, ossifying, fibroma, adenomatoid odontogenic tumor, a meloblastoma,and central arteriovenous hemangioma.Aneurysmal bone cyst, cherubism, fibrous dysplasia, giant cell tumor and brown tumor from hyperparathyroidism, in addition to being indistinguishable radiographically, also contain multinucleated giant cells [8,9].
Moreover, the neurofibromatosis type 1 syndrome and the Noonan syndrome can manifest at the level of maxillary similar lesions of CGCG [10]. The discriminant conditions that allow elaborating a final diagnosis are now discussed.
The aneurismal bone cyst is diagnosed by the identification of sinusoidal blood spaces within the tumor mass.
The giant cell tumor is distinctive from CGCG cases due to typical locations (the tumor is rare within the maxillary area) and histological characteristics: the giant cells of the tumor are distributed in a regular and uniform way, instead, in the granuloma, they are clumped in areas separated by virtually devoid areas. Fibrous dysplasia is characterized by the presence of “Chinese figure-like” trabeculae of woven or immature bone within a proliferating fibroblastic stroma. Besides these lesions, even for odontogenic keratocyst, odontogenic myxoma, odontogenic fibroma, ossifying fibroma, adenomatoid odontogenic tumor, ameloblastoma and central arteriovenous haemangioma, the definitive diagnosis occurs through histological examination [8, 9].
The root resorption index is useful to differentiate between CGCG and ameloblastoma; in the latter is more common compared to the former cases [22].
The brown tumor appears identical to CGCG in terms of histological and radiological conditions; the exclusion basis its foundations on the control of serum calcium values, phosphorous, alkaline phosphatise and kidney functionalities. Even the cherubism is microscopically indistinguishable from the CGCG. However, it usually recognizes, in the aftermath of its bilateral manifestation in juvenile patients, affected by this syndrome [8, 9].
The Granuloma characteristics in the histological examination
The CGCG, at the level of histological/diagnostical matters, is characterized by fibroblastic stroma at high cellular density, often myxoid, with plump, spindle-shaped cells with a high mitotic rate; there is a high vascular density, and there can be trabeculae’s bones [30, 31].
The multinucleated giant cells stand out in the fibroblastic stroma but are nevertheless abundant. They are usually irregularly distributed and are often localized at the level of hemorrhagic areas; morphology and dimensions vary according to each case, with several nuclei that can go from a few to several dozen.
At the periphery of the lesion, dystrophic calcifications and metaplastic ossifications are often presented [28, 29].
Different morphological parameters, including the index of mitotic activity, stromal characteristics, average dimensions of the multinucleated giant cells and percentages of occupied mass, have been tested in the attempt to correlate the histological aspect to the aggressive and non-aggressive CGCG behaviour. However, neither of those have shown a significant association according to the clinical behaviour of the lesion [8].
According to the following review, the CGCG radiological characteristics result to be a fundamental framework for the initial diagnosis but, not being specified, they are insufficient for the final diagnosis. In the clinical framework, it appears that is very important the histological exam to reach the final diagnosis, differentiating, likewise, the differential diagnosis.
Nevertheless, no correlation has been found between the aggressive degree outlined by the imaging response and the histological characteristics of the lesion.
Further studies at large-scales concerning the maxillary granulomatous giant cellular central cells could eventually generate useful data.
Authors declared no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
