
Case Reports | DOI: https://doi.org/10.31579/2643-6612/010
*Corresponding Author: Dr. Nilotpol Kashyap, Professor and Head, Department of Pedodontics and Preventive Dentistry, Universal College of Medical Sciences, Bhairahawa, Nepal
Citation: Kashyap N, Upadhyay M, Tripathi R, Pawar P, Sah RKP, et al. (2019) Central Giant Cell Granuloma. J Dent Oral Maxillofac Surg 2(2):dx.doi: 10.31579/2643-6612/010
Copyright: © 2019 Kashyap N. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 April 2019 | Accepted: 07 June 2019 | Published: 07 June 2019
Keywords: Keywords
Abstract
Central giant cell granuloma (central giant cell granuloma) is an uncommon benign bony lesion that occurs in the mandible and maxilla and accounts for approximately 7% of all benign tumours of the jaws [1]. The World Health Organization (WHO) has defined central giant cell granuloma as an intraosseous lesion consisting of cellular fibrous tissue that contains multiple foci of haemorrhage, aggregations of multinucleated giant cells and occasional trabeculae of woven bone [2]. Central giant cell granuloma occurs predominantly in children or young adults, with approximately 75%of cases presenting before 30 years of age although presentation can occur at any age [3]. Females are affected more frequently than males, with a ratio of 2:1 [4].
The clinical behaviour of central giant cell granuloma ranges from a slow growing asymptomatic swelling to an aggressive lesion that presents pain, local bone destruction, root resorption or tooth displacement [5].
Clinical Relevance
Chuong et al. [6] outlined the criteria that can be used to classify a lesion as aggressive or non-aggressive. Aggressive lesions are characterized by one or more of the following features: pain, paraesthesia, root resorption, rapid growth, cortical perforation, and a high recurrence rate after surgical curettage. Different authors have classified central giant cell granuloma into two types, based on clinical and radiographic features [5].
Aggressive lesions are mostly found in younger patients. Histologically there is no strict criterion to differentiate between aggressive and non-aggressive lesions, however the number and volume of giant cells versus other components of the lesion might give an indication on its clinical behaviour [7].
Surgery is considered the traditional treatment and it is still the most accepted one, however in literature not all authors agree on the type of surgery which should be performed. Excision via curettage has been associated with a low rate of recurrence for what concerns small lesions. In case of recurrences, curettage plus peripheral osteotomy and bone resection should be performed instead [7]. Unal et al. proposed obtaining safety margins by means of microdrilling of the surgical field with a diamond burr [8]. Although en bloc resection is the treatment which provides the lowest recurrence rate, only a few single case reports describe the use of this technique followed by reconstruction with iliac crest graft [7].
Non-surgical treatments (alpha interferon [a-IFN], calcitonin, corticosteroids) have been described and their benefits may be worthy of consideration. As pointed out by de Lange medical therapy success rates are still not reaching those of surgery in controlling the lesions and additional surgery is undoubtedly needed whenever medical therapy fails [9].
Case Report
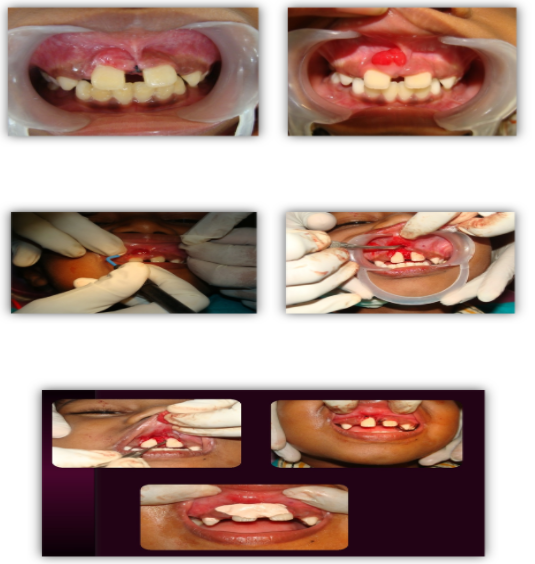
An 8 year old boy reported to the Department of Pedodontics and Preventive Dentistry, Rungta College of Dental Sciences & Research, Bhilai, Chhattisgarh with a chief complaint of swelling in upper front region of the mouth for the last 20 days, with a history of sudden increase in size since one week. Associated with swelling there was no history of pain or bleeding. On intra oral examination, a 1.5 × 1.5 cm, well defined oval, reddish pink, soft, non-tender, extending toward the palatal surface between the two central incisors. Diastema was present with respect to teeth 11 and 21. There was no associated lymphadenopathy. [Figure 1 showing preoperative view of patient; Figures 2a and 2b Showing the central giant cell granuloma].


No systemic abnormalities were detected. Hematological reports were noncontributory. A decision was thus made to excise the lesion. The growth was excised under local anesthesia with a cold scalpel. Care was taken to remove the entire base and the excised lesion was stored in 10% formalin and sent for histopathological examination. [Figure 3: Showing excisional biopsy].

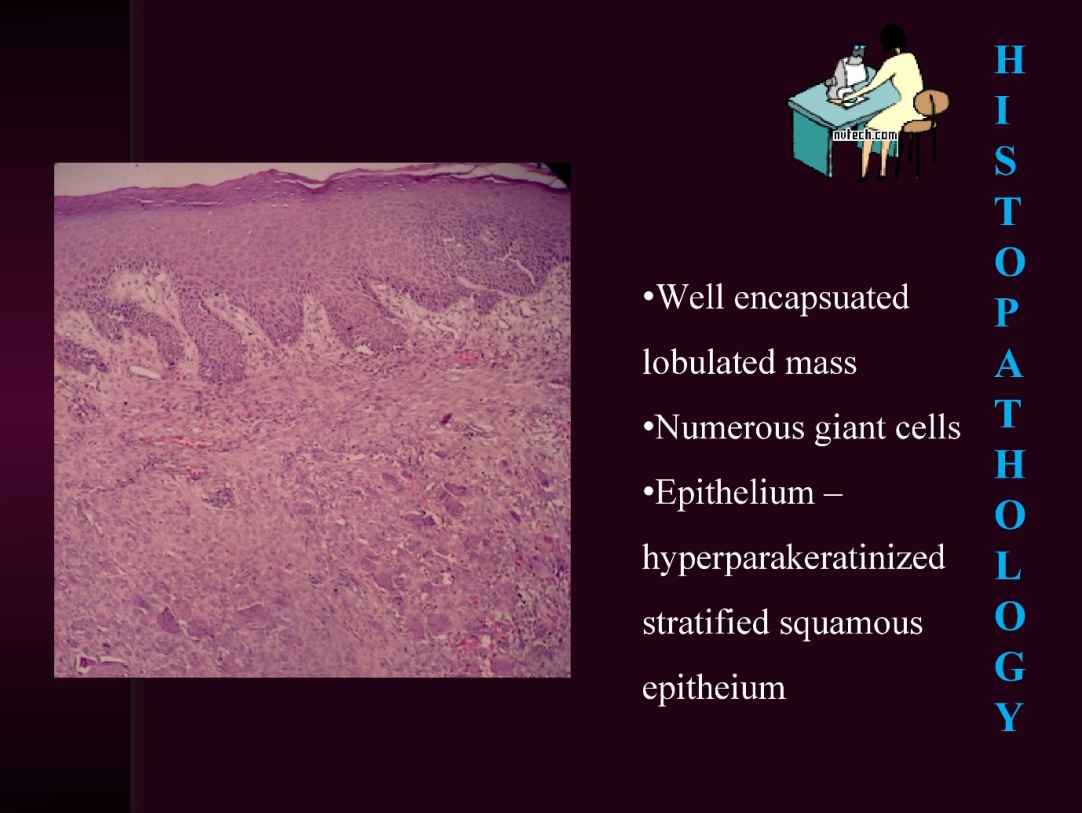
The histopathological section showed well encapsulated lobulated mass, numerous giant cells and hyperparakeratinized stratified squamous epithelium. The presence of these features was suggestive of central giant cell granuloma. The lesion reoccurs during 2nd week and 3rd month follow-up period and was retreated. The lesion did not reoccur during the 1-week and 6-month follow-up period. (Figures 4a and 4b Showing histopathological view); (Figures 5a-5e Showing retreatment of the recurrent central giant cell granuloma), (Figure 6 Showing postoperative view after retreatment).

The true nature of central giant cell granuloma remains speculative and considerable controversy exists in the literature. Normally, it is not considered an odontogenic lesion [10]. It has been suggested that it might be an inflammatory lesion, a reactive lesion, a true tumour, or an endocrine lesion [7]. One hypothesis suggests that central giant cell granuloma belongs to the spectrum of mesenchymal proliferative vascular primary jaw lesions11. As Vered et al. reported, the low mean microvascular volume (MVV) of Vascular Endothelial Growth Factor (VEGF)- and Basic Fibroblast Growth Factor (bFGF)-positive blood vessels implies little angiogenic activity, which contradicts the description of central giant cell granuloma as a true proliferative vascular lesion [10].
Central giant cell granuloma occurs predominantly in children or young adults, with approximately 75% of cases presenting before 30 years of age, however it really can occur at any age [3]. Kaffe et al. Stated that central giant cell granuloma is first seen at a mean age of 29.8 years and 60% of these lesions occur before the age of 30 [12]. Similarly, TOSCO et al., found that the age of the patients ranged from 7 to 80 years and only 10 patients (55.5%) were younger than 30 [7].
The most reliable factors which relate to an increased risk of recurrence include clinical activity of lesions (72% of recurrence in the aggressive forms, 3% of recurrence in the non-aggressive forms), young age, presence of perforation of cortical bone and tumour size [7].
de Lange et al. in his review analysed the different therapeutical options for central giant cell granuloma treatment [9]. Jacowayet al. [13] were the first to report on treatment with corticosteroids. Their mode of action is yet not fully understood: it is hypothesized that the extracellular production of bone-resorption-mediating lysosomal proteases by giant cells is inhibited by steroids which also induce apoptosis of the osteoclast-like cells.
An immunohistochemical study demonstrated that giant cells in central giant cell granulomas are osteoclasts through osteoclast-specific monoclonal antibodies staining [14]. It has also been demonstrated that giant cells in central giant cell granuloma express calcitonin receptors [15]. Calcitonin has also been hypothesized to directly inhibit giant cells. Harris et al. [16] first observed total remission of lesions in 4 patients affected by central giant cell granuloma. Similar results were reported by other authors. On the contrary Kaban et al. (1999) [17] observed a significant growth following calcitonin therapy. Recently Borges et al. (2008) [18] reported that calcitonin therapy provides an alternative to surgery in extended and aggressive lesions, despite the considerable amount of time taken up by the treatment itself. They experienced a reduction in size of the lesions but this therapy had to be complementary to surgery. There are many factors that can contribute to the various responses to calcitonin which have been reported in the literature [7]. Among these are: the different types of calcitonin (human, salmon) and the different types of administration (subcutaneous injections, nasal spray). One further aspect to take into consideration is the variable expression of calcitonin receptors which differs within central giant cell granuloma: receptors are not always present and immunohistochemical positivity is qualitatively diverse [19].
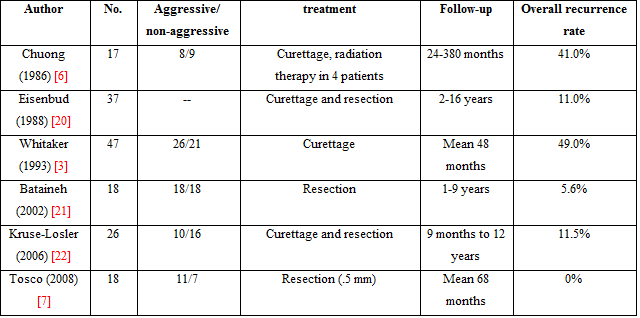
Currently, there are no biological markers to predict the clinical behaviour, and standard histological techniques are not helpful for the clinician to determine the prognosis. Surgery has always been considered to be the traditional treatment and it is still the most accepted. However, in the literature, not all authors agree on the type of surgery which should be performed. The treatment of central giant cell granuloma of the jaws is performed according to the following factors: aggressive versus non-aggressive behaviour, location, size and radiographic appearance. Surgical options range from large (en bloc resection) to more conservative approaches (curettage) [Table 1].
Background
Various authors proposed excision via curettage and the overall recurrence rate has been reported to range from 16% to 49% [3,6]. A higher incidence of recurrence was found in aggressive central giant cell granulomas and in younger patients, especially males. According to Eisenbud et al., in case of recurrence curettage plus peripheral ostectomy and bone resection should be performed [20]. Unal et al. proposed to obtain safety margins by means of microdrillingof the surgical field with a diamond burr [8]. However Eisenbudet al. [20] indicate that surgical curettage with peripheral osteotomy is still not the safest treatment for central giant cell granulomas, especially in aggressive lesions. En bloc resection might provide the greatest certainty of a cure: in a study of 18 patients with aggressive central giant cell granuloma, treatment consisted of en bloc surgical resection with a 5 mm margin of healthy tissue and only 1 patient had a recurrence [21].
In growing patients, aggressive surgical approaches are not a suitable solution for central giant cell granulomas. More conservative surgery is instead the only applicable strategy for subjects with deciduous dentition. In general destructive surgery (en bloc surgical resection with 5 mm margins) seems to be the safest option for the control of recurrences but it may result in facial deformities which are obviously of great concern.
Conflict of Interest: None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
