
Case Report | DOI: https://doi.org/10.31579/2690-4861/134
*Corresponding Author: M.M.Shokry, Department of Surgery, Anesthesiology & Radiology, Cairo University, Giza, Egypt.
Citation: A E Ashour, E A Berbish, A Osman & M M Shokry. (2021) Cecal lymphoma in a male Rottweiler dog. International Journal of Clinical Case Reports and Reviews. 7(5); DOI: 10.31579/2690-4861/134
Copyright: © 2021 M.M.Shokry, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 May 2021 | Accepted: 21 July 2021 | Published: 24 July 2021
Keywords: lymphoma; cecal diverticulum; weight loss; diarrhea
A 6-year-old male Rottweiler dog presented with a marked weight loss combined with abdominal pain and diarrhea over 3 month. Hematology revealed lymphocytosis, neutrophilia and eosinophilia. Abdominal ultrasound revealed a heteroechoic mid-abdominal mass with a focal hypoechoic area measuring 6.0 x 5.0 cm but with a confusing origin. The mass was resected and intestinal anastomosis was performed after celiotomy. Histopathology of the mass demonstrated massive lympho-proliferative lesions were diagnosed as low grade lymphoma with diffuse small lymphocytic (DSL-plasmacytoid) pattern. The dog was recovered and a one-month ultra sonography follow-up showed no-recurrence.
GI mesenchymal tumors are mainly comprised of a series of spindle cell tumors, including GI stromal tumors, leiomyomas, lymphomas, schwannomas, inflammatory fibroid polyps, fibromatoses and leiomyosarcomas (Greenlee et al., 1990; Teske et al., 1994; Davis et al, 2000; Miettinen and Lasota, 2001). Changes in classifications of GI tumors have emerged due to recent advances in immunohistochemistry and electron microscopy since GI stromal tumors in about 95% of cases stain positively for the protein CD117 (Day et al, 2003; Giuly et al.,2003). Differing between benign and malignant GISTs may develop few problems however, GISTs may appear benign both in mitoticcounts and lack of cellular atypia, but still behave malignantly (Miettinen et al, 2002). GISTs smaller than 3 cm are generally considered benign tumors (Bonsaing et al., 2007) and GISTs larger than 3-5 cm, with mitotic counts greater than 2/10 high power field or that involved more layers are generally considered high-risk tumors for malignancy ( Giuly et al, 2003; Miettinen et al, 2000).The presented case is reported due to its rare occurrence.
A 45 kg, 6-year male Rottweiler was attended at the surgery clinic of the faculty of Veterinary Medicine,Cairo University, with a history of anorexia, lethargy, cachexia, weight loss, abdominal pain and diarrhea( over 3 month period). Vomiting and seizures were not reported. Vaccinations were up to date and housed mainly indoors, with some time spent out.
Clinical examination
At physical examination,the dog was alert with normal temperature, pulse and respiration, pale mm, and palpation of the abdomen and lymph nodes were normal. Blood sample was collected for complete blood count (CBC), serum biochemical analysis for liver and kidney functions, serum amylase and lipase values for pancreatic lesions and blood parasites. An abdominal ultrasound and thoracic radiographs were performed for any pathological lesions.
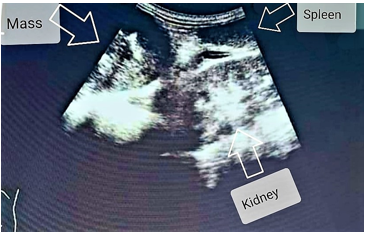
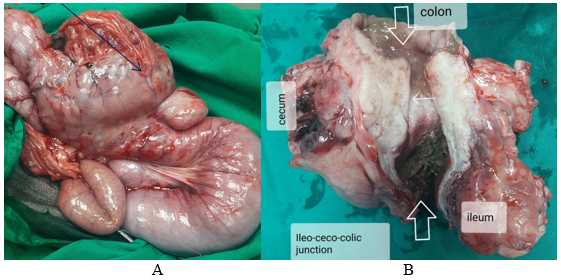
CBC showed moderate leukocytosis with absolute neutrophilia (41.80%), lymphocytosis (41.40%), monocytosis (10.60%) and eosinophilia (4.08%). Serum biochemical analysis was within the normal range. Examination for blood parasites was negative. Thoracic radiology showed no pathology. Abdominal ultrasonography detected a heteroechoic mid-abdominal mass with a focal hypoechoic area measuring 6.0 x 5.0 cm but with confusing origin (fig.1).The remainder of the intestinal tract and viscera were unremarkable. Neither lymph adenopathy nor free fluid were noted. Surgical abdominal exploration under general anesthesia revealed an invasive mass at the ileo-cecal junction. The mass including the involved part of the intestine was resected with subsequent intestinal anastomosis. The abdomen was lavaged with sterile saline solution. The anastomosis site was omentalised and the abdominal wall was closed routinely. The enucleated mass including the resected intestinal part was fixed in 10% formol saline and submitted for histopathology (Fig.2 A &B).The dog postoperative recovery was uneventful and kept under supportive and antibiotic therapy for one week. Clinical and ultrasonography follow-up one month later showed no evidence of mass reccurence.
Histopathological examination
Tissue specimens from tumor mass and intestinal segment were fixed in 10% neutral buffered formalin. The fixed specimens were then trimmed, washed and dehydrated in ascending grades of alcohol, cleared in xylene, embedded in paraffin, sectioned at 4-6U thickness and stained by hematoxylin and eosin were used (Bancroft et al.,2013).
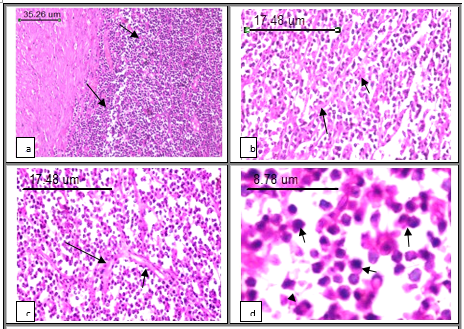
Massive lymphoproliferative lesions were diagnosed as low grade lymphoma with diffuse small lymphocytic (DSL-plasmacytoid) pattern. The histological section dominated a monotonous morphology of the tumour cell population, mainly composed of uniform small oval tumour cells. The tumour mass was closely attached to external muscular layer of the intestinal wall forming bulky nodular formation containing uniform, small-sized cells. The architecture is diffuse, the mitotic index is low and mitoses may not be observed. The nuclei appeared the same size as a canine erythrocyte and uniformly round. The chromatin pattern was coarsely aggregated. Nucleoli were absent or there may be one small, usually central nucleolus. The cytoplasm was usually scant and poorly staining. In this case histological sections demonstrated a diffuse homogeneous population of small cells with low mitotic rate and plasmacytoid differentiated cells. A centrocytoid population of cells with eccentrically localized basophilic nucleus and adjacent layer of lighter cytoplasm resembling to plasma cells. The stroma consisted of fine sinusoids, or fine reticular networks with unique, visible trabeculae (Fig. 3).
According to clinicohistopathological data,the definitive diagnosis of the presented case is low grade lymphoma with small lymphocytic pattern. With respect to the patient’s presented reported signs, there were crampy abdominal pain associated with anorexia, bloating, diarrhea and weight loss. Almost similar signs have been reported in dogs with stromal intestinal tumors (Frgelecova et al, 2013; Maia et al., 2009; Greenlee et al., 1990; Greenlee 1988). Although most dogs with lymphoma are characterized by the presence of non-painful periphera lymphadenopathy (Greenlee et al., 1990), the present case showed normal peripheral lymph nodes. Hematology revealed neutrophilia, lymphocytosis, monocytosis and eosinophilia which indicate intense inflammatory response.
The histological grades of canine lymphomas were classified as low (small lymphocytic or centrocytic lymphomas) or intermediate to high (diffuse large cell, centroblastic, and immunoblastic lymphomas) (Greenlee et al., 1990). Clinical staging is an important factor in predicting survival and response to treatment in man (Lieberman et al., 1986). The present case was diagnosed as low grade lymphoma which is rarely noticed in dogs and usually goes unrecognized by most owners with improved survival rate while almost all dogs may have advanced grades (intermediate or high) (Madewell 1975). Treatment was by surgical exicision of the lesion and intestinal anastomosis without chemotherapy since ultrasonographic examination follow-up for one month indicated no recurrence.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
