
Case Report | DOI: https://doi.org/DOI: 10.31579/2690-4861/126
1 Faculty of Medicine and Biomedical Sciences, University of Yaoundé I, Cameroon.
2 Ophthalmology Unit, Yaoundé Gynaeco-Obstetric and Pediatric Hospital, Cameroon.
3 Ophthalmology Unit, Yaoundé Central Hospital, Cameroon.
*Corresponding Author: Chantal Nanfack Ngoune, Ophthalmology unit, Yaoundé Gynaeco-Obstetric and Pediatric Hospital, Cameroon.
Citation: Chantal N Ngoune, A Nomo, Zoua MEA, Caroline M tsimi, W Nzokou. (2021) Cavernous sinus thrombophlebitis caused by a dental infection: A case report. International Journal of Clinical Case Reports and Reviews. 7(4); DOI: 10.31579/2690-4861/126
Copyright: © 2021 Chantal Nanfack Ngoune, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 March 2021 | Accepted: 28 June 2021 | Published: 01 July 2021
Keywords: Cavernous sinus; thrombophlebitis; dental infection; computed tomography; dental cellulitis; case report
Septic cavernous sinus thrombosis (CST) is a rare, life-threatening complication of infections of the face; it is commonly caused by methicillin–resistant Staphylococcus aureus and anaerobes. The need of an early diagnosis and appropriate treatment is very important. We report the case of a 67 years old woman, referred by the dentist for left eye ptosis associated with dental cellulitis. Prior to her consultation at the dentist, she had presented with a headache, fever, painful swelling of the left maxilla. On clinical exam, there was proptosis, chemosis, ophthalmoplegia and hypoesthesia of the trigeminal nerve. Orbitocerebral contrast enhanced Computed Tomography (CT) showed grade 1 proptosis, hypodensity, dilatation of the lateral wall of the cavernous sinus and enlargement of the superior ophthalmic vein suggesting thrombosis. She was placed on empiric broad-spectrum antibiotherapy and progress was marked by improvement of her condition within 21 days of treatment. This case emphasized the multidisciplinary approach including the radiologist, the dentist, and the ophthalmologist. The need for dental care and the early and adequate management with antibiotics of any infection of the face should be considered.
Septic cavernous sinus thrombosis (CST) is a rare, life-threatening complication of infections of any of the tissues drained by the cavernous sinus such as the mid-face, orbit and sinuses [1]. With the introduction of antibiotics, the mortality and morbidity rates have significantly reduced although they remain high [1, 2]. The necessity of an early diagnosis and appropriate treatment is therefore of great importance. Clinical presentation includes proptosis, chemosis, ocular motor nerve palsy, and sensitive disorders. Imaging investigations, such as contrast enhanced computed tomography (CT) and magnetic resonance imaging (MRI) have had a significant impact on the diagnosis [3]. This condition is rare and after literature review, we found very few case series and some cases reports. We herein share a case of cavernous sinus thrombophlebitis caused by a dental infection.
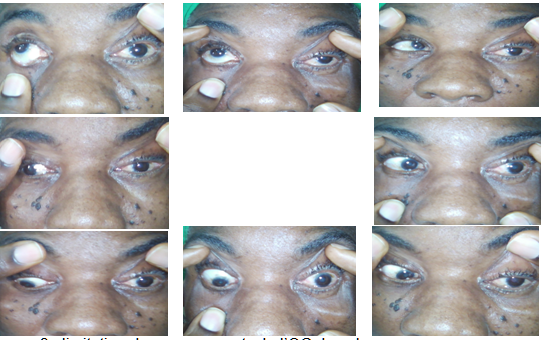
A 67 years old woman, referred by the dentist for the management left ptosis associated with dental cellulitis. Her history revealed the presence of headache, fever and painful swelling of the left maxilla a week prior to the sudden onset of left ptosis. On admission the patient was well oriented and alert. Ophthalmological examination revealed a left complete ptosis (fig1), proptosis, chemosis, total ophthalmoplegia (palsy of the oculomotor, trochlear and abducens nerves) (fig2) as well as a non-reactive pupil, hypoesthesia of the ophthalmic and maxillary divisions of the trigeminal nerve and an anomaly of the left corneal reflex. The intraocular pressure, anterior chamber and fundus exam were normal for both eyes. Laboratory tests showed a leukocyte count of 11200/mm3, C-reactive protein (12.0 mg/dl) and blood sugar (1.02 g/l). Orbitocerebral contrast enhanced CT showed grade 1 proptosis, hypodensity and dilatation of the cavernous sinus lateral wall and enlargement of the superior ophthalmic vein indicating thrombosis (fig3). The clinical and paraclinical evidence were in favor of a cavernous sinus thrombophlebitis. The patient was treated with systemic antibiotics; Cefuroxime, 1 g per day and Metronidazole, 1.5 g per day for 21 days. This was done alongside dental care. Progress was marked by the absence of fever, headache, and swelling of the left maxilla. There was progressive regression of ptosis, ophthalmoplegia (fig 4), and the onset of binocular diplopia, which was treated with right eye occlusion. After 21 days of antibiotics, the patient was fully recovered.



The two cavernous sinuses are complex structures due to their location at the base of the skull and due to the presence of vascular and nerve fibers crossing them. All facial cavities are drained into the cavernous sinus, and therefore any disruptions occurring in this area may lead to vascular thrombosis and the compression of nerve fibers.
CST is a rare but life-threatening condition; the mortality rate remains high between 20 and 30 % with the use of antibiotics. [4] Factors associated with morbidity include residual cranial nerve palsies and visual impairment. In 95% of cases, CST occurs as a complication of infections, mainly sinusitis and particularly sphenoid and ethmoid sinusitis. This is followed by skin infections of the face, loco-regional infections such as otitis and dental infections (just like the case of our patient) found in 10% of CST’s [5].
The spread of bacteria from the oral cavity from dental infections to the cavernous sinus is made possible from the orbit through the pterygopalatine space or the pterygoid plexus or facial veins hematogenously [3, 6].
A typical clinical presentation combines signs of impairment of the vascular and nerve fibers crossing the cavernous sinus (sympathetic, III, IV, V1, V2 and VI) and signs of upstream stasis of the thrombosed sinus (chemosis, exophthalmos, eyelid edema). The diagnostic timeframe is usually less than a week and the triad includes chemosis, ptosis and painful ophthalmoplegia with hypoaesthesia and / or paresthesia in the areas of V1 and V2. Eyelid edema and exophthalmos are usually associated with this clinical picture [1, 4]. If visual acuity is reduced, the fundus will generally show papilledema. The main associated general signs are fever and headache, which precede local signs [1, 4]. Psychomotor slowdown and meningeal syndrome should suggest a complication.
Contrast enhanced CT and MRI can confirm the diagnosis of CST, rule out differential diagnosis, and may reveal the primary source of infection. The direct signs on CT include heterogeneous filling defect of the cavernous sinus indicating the local presence of a thrombus and convex shaping of the lateral wall. The indirect signs are dilatation of the superior ophthalmic vein and exophthalmos [6]. On MRI, direct signs include changes in signal intensity, size and contour of the cavernous sinuses; indirect signs are dilatation of the ophthalmic vein, exophthalmos and increased dural enhancement along the lateral border of the cavernous sinuses. [6-8]. Up to date, there is no consensus about primary imaging modalities concerning the use of MRI or CT for the diagnosis of CST. Some authors preferred contrast-enhanced CT to contrast- enhanced MRI while others preferred MRI to CT [7]. However, we used CT for our patients because of its accessibility and the cost in our setting. The most common pathogens in CST related to dental infection are staphylococcus aureus found in 60% to 70% of cases followed by Streptococcal sp., gram-negative bacilli and anaerobes [5, 6]. In our case, we were not able to identify a specific pathogen, so we used broad-spectrum antibiotics; cefuroxime and metronidazole. After 21 days, we obtained favorable results. The consensus on treatment of CST is the systemic use of high dose antibiotics covering methicillin–resistant Staphylococcus aureus and anaerobes such as penicillins, third –generation cephalosporins or carbapenems administered for at least two weeks beyond the time of clinical recovery to prevent any recurrence [5,6,9]. Surgery of the cavernous sinus is usually not recommend. There is some controversy on the use of anticoagulants in association with antibiotics to treat CST. Levine et al. in their review found no conclusive evidence for reduced mortality in patients treated with anticoagulants but they found a reduced morbidity [10]. However, others authors still recommend adding anticoagulants to therapy [1, 11, 12, 13]. Southwick et al. in a review of 86 reported cases, 28 patients were placed on heparin, and the mortality rate was lower in this group [13]. A few cases of systemic hemorrhage were reported [6], but this study was based on a retrospective series and review in the absence of a clinical trial on this subject. The use of corticosteroids is not very clear. They can be effective for the improvement of cranial nerve palsies but an important side effect is immunosuppression that can worsen the infection. The prognosis of CST remains poor despite the introduction of antibiotics. Intracranial extension of infection and thrombosis are the leading complications of CST which may result in optic neuropathy, retinal vessel occlusion, meningitis, encephalitis, brain abscesses, pituitary infections, subdural empyemas, intracavernous carotid aneurysms, and thrombosis of other sinuses [5, 6], thus a high mortality and morbidity rate of 20-30%.
Cavernous sinus thrombophlebitis caused by a dental infection is a rare and life threatening condition. The diagnostic triad includes ptosis, chemosis and painful ophthalmoplegia. Imaging confirms the diagnosis, and management includes broad-spectrum antibiotherapy combined with dental care.
Ethics approval: Recruitment of participant was done at free will and an informed consent form was signed.
Conflict of interest: None.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
