
Review Article | DOI: https://doi.org/10.31579/2641-5194/048
*Corresponding Author: Martynov Vladimir Leonidovich, Doctor of Medical Sciences, Associate Professor, National Research Nizhny Novgorod State University, Russia.
Citation: Martynov Vladimir Leonidovich (2021) Causes of Duodeno-Gastric Reflux as a Surgical Problem. J, Gastroenterology Pancreatology and Hepatobilary Disorders. 5(6); DOI: 10.31579/2641-5194/048
Copyright: © 2021, Martynov Vladimir Leonidovich, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 April 2021 | Accepted: 10 September 2021 | Published: 23 September 2021
Keywords: prevention of stomach cancer; duodeno-gastric reflux; chronic violation of duodenal patency; indications for surgery
The author points to duodeno-gastric reflux as gastric precancer. In the overwhelming majority of patients, GHD is caused by compression of the lower-horizontal part of the duodenum by the superior mesenteric artery.
The duodenum (12-PC), located in a kind of vascular fork (Figure 1) formed by the superior mesenteric artery (SMA) and the aorta, under certain conditions can be compressed by the SMA or one of its branches, causing arterio-mesenteric compression (AMC) bottom horizontal part 12-PC. which leads to the development of a mechanical form of chronic disorders of duodenal patency (CPD), duodeno-gastric reflux (GDR), which is assumed to be a precancerous state.

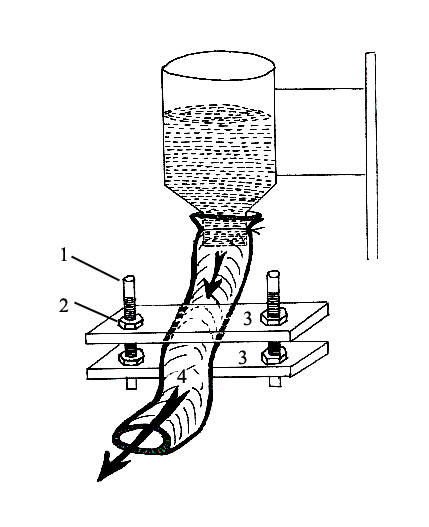
The main pathogenetic factors in the development of stomach diseases in chronic disorders of duodenal patency (CPD) are duodenogastric reflux (DGR) and motor-evacuation disorders of the stomach [1]. Many authors consider GHR as a factor in the formation of chronic gastritis [3], gastric ulcer and 12 duodenal ulcer [1], and stomach cancer [1, 2, 3, 4]. Duodenal hypertension, due to both mechanical and functional reasons, plays a leading role in the occurrence of GHD in patients with chronic cerebrovascular disease [1, 2]. Damage to the gastric mucosa by the thrown duodenal contents, which includes bile acids and lysolecithin, is considered the main cause of gastric ulceration and cancer [1, 2, 3, 4]. This opinion is confirmed experimentally and by clinical observations. Recognizing the presence of HNDP and the need for its correction with therapeutic measures or surgery, the indications for correction methods, indications for each individual patient are not defined. In the experiment, we tried to find out the degree of arteriomesenteric compression (AMC), when there is a violation of patency in the duodenum. Creation of a model of various degrees of arteriomesenteric compression of the lower-horizontal part of the duodenum with the determination of the passive flow rate of the experimental fluid. To reveal the role of the AMK degree for passive flow through the small intestine of a human corpse, we have created a model of AMK as one of the forms of HNDP in the pathological hall. The system of the AMK model is as follows (Figure 2): on two screws (1), two strips (3) are fixed with nuts (2). When moving the nuts (2) along the axis of the screw (1), the upper bar also moves, which changes the distance between the bars. The distance between the slats mimics the distance between the aorta and the VMA, i.e. AMK degree. A section of the small intestine with a diameter of 2.5 cm and a length of 35-40 cm was placed between the slats (4). The proximal end of the intestine was put on a 2.5 cm neck of a cut-bottom plastic bottle. The neck of the bottle was fixed at a height of 10 cm from the slats on a tripod. A constant volume (500 ml) of liquid with a certain viscosity (machine oil) was poured into the bottle.
Experience 1. Determined the distance between the bars, equal to the diameter of the neck of the bottle - 2.5 cm. 500 ml of the experimental liquid passed through the intestine in 5.5 seconds, which was taken as 100%.
Experiment 2. Determined the distance between the bars (AMC degree) of 2 cm. The experimental liquid (500 ml) passed through the intestine also in 5.5 seconds (100% of the initial time).
Experiment 3. Determined the distance between the bars (degree of AMK) of 1.5 cm. The experimental liquid (500 ml) passed through the intestine in 7.5 seconds (140% of the initial time).
Experience 4. Determined the distance between the bars (AMC degree) in 1.0 cm. The experimental liquid (500 ml) passed through the intestine in 9 seconds (170% of the original time).
Experiment 5. Determined the distance between the strips of 0.5 cm. The experimental liquid (500 ml) passed through the intestine in 28.7 seconds (420% of the original time).
Determination of the distance between the aorta and the superior mesenteric artery at the level of the lower horizontal part of the duodenum in patients with reflux disease.
Signs of colonic, duodeno-gastric, gastroesophageal reflux were observed in each patient in 94% of patients. Therefore, in the concept of reflux disease, we combine simultaneously reflux of all three levels.
When determining the specified distance, 129 patients received following results:
AMC = 5 mm - in 17 (13%) patients;
AMC = 6-10 mm - in 47 (36%) patients;
AMС = 11-15 mm - in 31 (24%) patients;
AMС = 16-20 mm - in 26 (20%) patients;
AMС = 21-25 mm - in 4 (3.5%) patients;
АМС > 25 mm - in 4 (3.5%) patients.
Various degrees of compression of the lower-horizontal part of the 12 PC between the aorta and the superior mesenteric artery are shown on computed tomographic images after computed tomography (Figure 3).
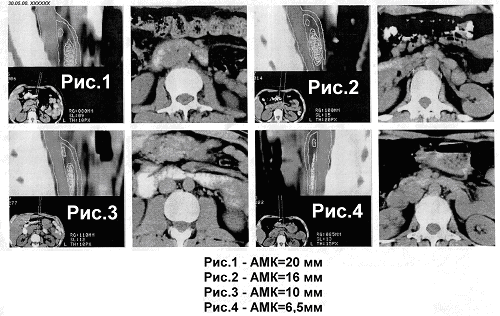
On CT scans, an increase in the degree of compression is clearly visible in the form of a decrease in the lumen of the lower-horizontal part of the 12th PC between the aorta and the MCA as the distance between these vessels decreases.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
