
Review | DOI: https://doi.org/10.31579/2768-0487/180
1Medical Microbiology Department, College of Health Sciences, Hawler Medical University.
2Midwifery department, Erbil technical medical institute, Erbil polytechnic university, Kurdistan region/Erbil/ Iraq.
3Department of Biology, College of Education, Salahaddin University-Erbil, Kurdistan Region, Iraq.
4Medical Laboratory Technology Department, Kalar Technical College, Garmian Polytechnic University, Kalar, Iraq.
*Corresponding Author: Fattma A. Ali., Medical Microbiology Department, College of Health Sciences, Hawler Medical University.
Citation: Al-Daoody AA, Hero H. Abbas, Fattma A. Ali, Media A. Othman, Sawsan M. Sorche, et al., (2025), Causative Agents of Primary Amoebic Meningoencephalitis Naegleria Fowleri, Journal of Clinical and Laboratory Research, 8(3); DOI:10.31579/2768-0487/180
Copyright: © 2025, Fattma A. Ali. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 June 2025 | Accepted: 18 June 2025 | Published: 30 June 2025
Keywords: free-living amoebae; primary amoebic meningitis; naegleria; diagnosis; pathogen
The free-living amoeba Naegleria fowleri is frequently found in humid freshwater settings including warm springs, lakes, naturally occurring mineral water, and resort spas that are frequented by travelers. Primary amoebic meningoencephalitis (PAM), a severe, deadly illness of the central nervous system that kills a person within seven days, is caused by Naegleria fowleri. When ameba-containing water come into the body through the nose, commonly during re-creational aquatic actions like swimming or diving, infection may result. The PAM Though it was once believed to be an uncommon disorder, more instances are being documented every year. PAM is challenging to detect as its signs and symptoms resemble those of meningitis caused by bacteria. Therefore, the first step for identification is clinical inference and clinician attention. Therapy must start as soon as amoebae are found in CSF wet mount and involve systemic and intrathecal injection of large doses of amphotericin B, either with or without miconazole, rifampin, and sulfisoxazole. The spread of N. fowleri can be stopped via adequately chlorinating heavily used swimming pools (one part per million). In high-risk locations, local public health authorities should also think about monitoring waters used for recreation for N. fowleri, especially in summertime. This review is meant to bring focus to the significance of Naegleria fowleri infections and provides information on ways to comprehend the disease's pathogenesis, clinical symptoms, and associated processes, in addition to treatment and prevention measures.
The ameboflagellate known as Naegleria fowleri is referred to as "the brain-eating amoeba"(Gyori, 2003). This amoeba thrives in tropical and subtropical environments because it is thermophilic. Its development is facilitated by warm water from power plants or elevated temperatures during the sweltering summer months (Martinez and Visvesvara, 1997). Primary amoebic meningoencephalitis (PAM) is a severe, active, and quickly lethal central nervous system (CNS) infection caused by this amoeba. The infection is brought on by trophozoite breathing (Gyori, 2003). After inhaling contaminated water, it clings to the olfactory nerve before moving down the fila olfactory and blood vessels through the cribriform plate of the ethmoid bone and into the anterior cerebral fossae. It consumes nerve tissue, causing massive bleeding, necrosis, and inflammation that eventually results in fatality (Control and Prevention, 2008). Children and young adults in good health who have recently come into contact with lukewarm freshwater water (polluted water found in ponds, swimming pools, and artificial lakes) are susceptible to infections. Ameba has also been found in industrial water sources that are artificially treated (Huizinga and McLaughlin, 1990), as well as in home water systems There have been around 310 instances documented, with a in elevation case mortality rate of almost 95% (Cervantes-Sandoval et al., 2008, Gautam et al., 2012). In recent years, PAM instances have been recorded more often globally. The rise in occurrence might perhaps be attributed to heightened knowledge of the illness or the advancement of more quick, extremely precise, sensitive, and specific diagnostic procedures, such PCR. Changes in the environment, thermal contamination of water from industry, and the growth of industrialized areas with cooling towers and nuclear power plants may also provide more opportunities for infection. These factors allow for the simultaneous growth of amoeba and their bacterial food source (Marciano-Cabral and Cabral, 2007). This review aimed to focus the role of N. fowleri as a causative agent of meningitis to draw special attention for its analysis and organization.
2.Ecology of Naegleria fowleri
The genus Naegleria is found in water as well as soil all around the world (De Jonckheere, 2012). Additionally, they have been kept far from sewage, aquaria, fresh and warm-water lakes, streams, spas, overheated but non-chlorinated swimming pools, hot-spring hydrotherapy and therapeutic pools, as well as healthy people's throats and nasal cavities (Trabelsi et al., 2012). In addition, this amoeba has been isolated from a variety of species, include fish, amphibian species, and reptiles (Pantchev and Tappe, 2011). 012This microorganism's susceptibility to high concentration is shown by the fact that it has not been found in saltwater. Since the existence of cyanobacteria and eubacteria has been linked to the vertical dispersion of N. fowleri in water, it is plausible that the Naegleria genus's natural purpose is to regulate populations of bacteria. Furthermore, the amounts of manganese and iron in the water column have been linked to the dispersion of Naegleria (Martínez-Castillo et al., 2016). Because it is thermophilic, N. fowleri can withstand temperatures as high as 45C˚.As a result, during the summer, when the outside temperature is expected to be high, these amoebae mostly multiply (Sifuentes et al., 2014).
3.Life Cycle of Naegleria fowleri
Depending on the surroundings, this protozoon goes through three distinct phases in its life cycle (Siddiqui et al., 2016). The flagellate, cyst, and trophozoite stages (cystSt). The trophozoites of ameboids range in size from 10 to 25 mm and reproduce by binary fission. In nutrient-poor aquatic settings or when the media's ionic content shifts, the trophozoites can transition into the flagellate phase. Unfavorable settings, such as high temperatures, low pH environments, or high salt levels, can be home to the cystSt of N. fowleri. (Stahl and Olson, 2021). In its life cycle, N. fowleri goes through three stages: cysts, trophozoites, and flagellated stages. Promitosis is the process by which trophozoites multiply (nuclear membrane stays intact). Fresh water, soil, thermal discharges from power plants, heated swimming pools, hydrotherapy and therapeutic pools, aquariums, and sewage are all known to contain Naegleria fowleri. When trophozoites encounter unfavorable environmental conditions, including a decreased food supply, they can transition into a transient, non-feeding, flagellated stage (10–16 µm in length). When favorable circumstances are restored, they transition back to the trophozoite stage. Cerebrospinal fluid (CSF) and tissue contain Naegleria fowleri trophozoites, with flagellated forms infrequently seen in CSF. Brain tissue doesn't have cysts. The ameba or flagellate will develop a cyst if the environment is not favorable for continuous feeding and growth (such as low temperatures, food scarcity). The cyst form has a spherical diameter ranging from 7 to 15 µm. It features a single nucleus and a smooth, one-layered wall. Because they can withstand harsh environments longer, cysts have a higher chance of surviving until they do (Yoder et al., 2010a) (Figure 1).
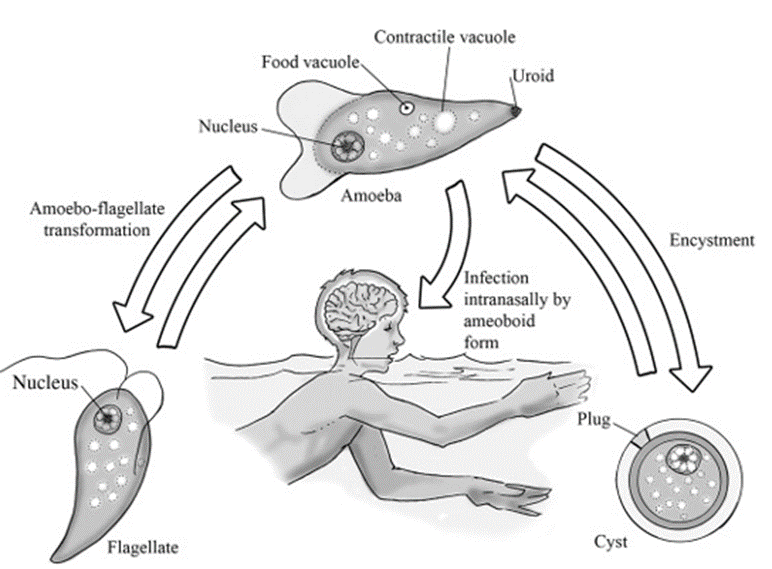
Figure 1: Lifespan series of Naegleria fowleri (David and AP, 2006).
4.Pathogenesis
Second only to HIV infection, protozoal infections of the central nervous system (CNS) are important global sources of morbidity and mortality (Mishra et al., 2009). N. fowleri causes infection of the central nervous system by means of amoebae that enter the nasal cavity, pierce the olfactory neuroepithelium, migrate along the olfactory nerves, traverse the cribriform plate, and eventually arrive at the olfactory bulbs (OBs) (Figure. 2 a) (Rojas-Hernández et al., 2004). After the amoebae enter the brain, they can multiply and cause an acute inflammatory response (Figure 2b), which can cause the patient to pass away in about a week. (Cervantes-Sandoval et al., 2008). Over ninety percent of N. fowleri infections are caused by persons splashing, diving, or submerging themselves in warm water bodies, which opens the nasal cavity to the
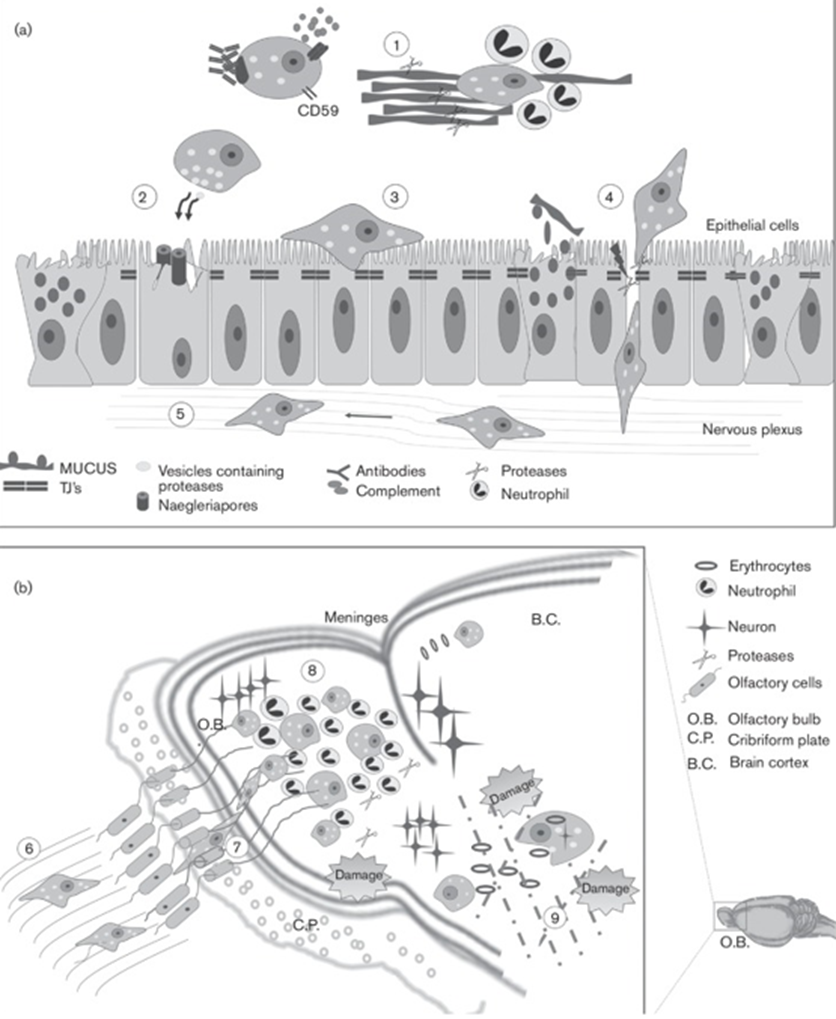
Figure 2: Diagram illustrating the infection caused by N. fowleri. (a) The preliminary phases of PAM. (1), evade the innate immune system; (2) cause independent-contact cytotoxicity (naegleriapores); (3) adhere to epithelial cells; (4) invade the neuroepithelium; and (5), migrate to OBs. (b) The latter PAM phases. (6) Olfactory phylum contact; (7) amoeba cribriform plate crossing; (8) N. fowleri proliferation and inflammatory response in the OBs; and (9) tissue injury (bleeding, phagocytosis, and protease release) (Martínez-Castillo et al., 2016).
Amoeba's trophozoites (Grace et al., 2015a). While recreational swimming activities are the primary source of infection, religious organizations' ablution procedures and the use of hygiene equipment such as neti pots can also cause the illness (Siddiqui et al., 2016). It has also been proposed that the amoeba can "dry-infect" through dust that contains cysts, which will lead to infection after the amoeba transforms into its trophozoite form. Even while this last process only accounts for around 6.5% of PAM instances, it is quite worrying because there isn't much that can be done to stop dust from entering the lungs (Maciver et al., 2020). The amoeba enters the nasal canal, enters the nasal mucosa, and then travels through the cribriform plate, following the olfactory nerves until it reaches the olfactory bulb. Following its entry into the brain by the olfactory nerve bundles, it grows and finally results in cerebral edema, herniation, and death (Pugh and Levy, 2016). Infections with N. fowleri have been reported in otherwise healthy children and adults after engaging in water sports including swimming, diving, and water skiing. Additionally, it has been hypothesized that when water is driven or splashed into the nasal cavity, it enters the host's body through the nose. In order to reach the olfactory bulbs inside the central nervous system (CNS), infectious agents first adhere to the nasal mucosa and then move down the olfactory nerve and through the cribriform plate, which is more porous in children and young adults (Jarolim et al., 2000). When N. fowleri enters the olfactory bulbs (Figure3), it triggers a powerful immunological response by stimulating neutrophils and macrophages in the innate immune system. Trophozoites are the form in which N. fowleri enters the human body. The trophozoite's feeding cups are structures on its surface that allow the organism to consume human tissue, fungus, and bacteria (Marciano-Cabral and Cabral, 2007). The pathogenicity of N. fowleri is based on the production of cytolytic chemicals, such as acid hydrolases, phospholipases, neuraminidases, and phospholipolytic enzymes that contribute to host cell and nerve damage, in addition to tissue degradation by the feeding cup. Because N. fowleri may live freely in soil, water, or its host, the human central nervous system (CNS), it is an amphizoic amoeba. The pathogenicity of N. fowleri is based on the production of cytolytic chemicals, such as acid hydrolases, phospholipases, neuraminidases, and phospholipolytic enzymes that contribute to host cell and nerve damage, in addition to tissue degradation by the feeding cup (De Jonckheere, 2011). Histology reveals an acute inflammatory response mostly consisting of neutrophils with several trophozoites present and large regions of lytic necrosis. The literature shown that the fibrinopurulent exudate is essentially nonexistent in human and experimental animal models (Guarner et al., 2007). In order to visualize motile N. fowleri, a microscopic analysis of freshly obtained cerebrospinal fluid (CSF) is typically used to provide a quick diagnosis. Giemsa or Wright stains of CSF smears in conjunction with the enflagellation test can be used to identify trophozoites. These two approaches may be sufficient in the beginning as a prompt diagnosis is required to initiate an appropriate course of treatment. The anti-N. fowleri antibody immunofluorescence test (Movahedi et al., 2012).
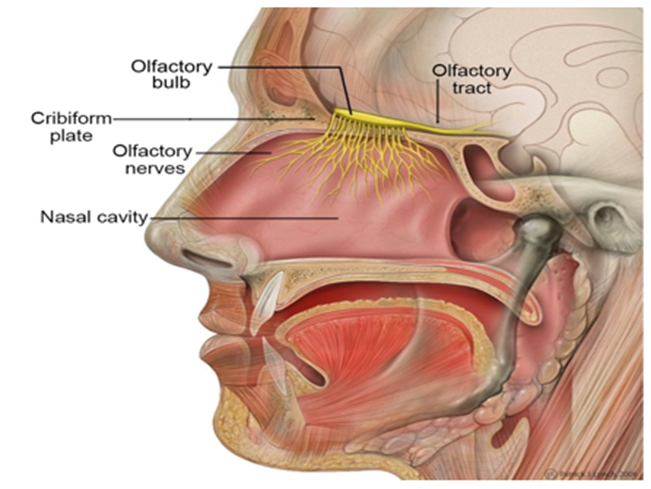
Figure 3: The olfactory nerve and olfactory bulb are emphasized in the head anatomy. This neural pathway is the main route via which the amoebas enter the brain (Gillen et al., 2019).
5.Primary Amoebic Meningoencephalitis (PAM)
The uncommon but almost usually deadly disease known as primary amoebic meningoencephalitis (PAM) is brought on by an infection with the free-living, thermophilic amoeba Naegleria fowleri, which is prevalent in freshwater habitats (Marciano-Cabral and Cabral, 2007). PAM develops in otherwise healthy people who come into contact with heated, untreated, or inadequately disinfected water. When N. fowleri-containing water enters the nose, it causes infection. The amoebae then migrate through the cribriform plate and go via the olfactory nerve to the brain. There is a range of 2 to 15 days during the incubation period. Similar to those of bacterial or viral meningitis, signs and symptoms of infection might include fever, headache, stiff neck, anorexia, vomiting, altered mental state, seizures, and coma. Usually, death happens three to seven days after symptoms appear. Acute hemorrhagic necrosis of the cerebral cortex and olfactory bulbs is revealed by autopsy results (Yoder et al., 2010b) Despite the fact that Naegleria has over forty species, PAM is only caused by a single of them, N. fowleri. In the hottest periods of the year, when the outside temperature rises, N. fowleri may thrive in natural bodies of water, such as lakes and rivers, and can withstand temperatures as high as 45°C. Normally free-living, N. fowleri feeds on waterborne bacteria; inadvertent entry of the amoeba into the human nostril causes PAM. Water samples from freshwater lakes, ponds, and rivers have shown evidence of N. fowleri. These samples also came from soil, hot springs, warm groundwater, and thermally contaminated water (Maclean et al., 2004). The free-living ameba Naegleria fowleri causes a quickly progressing and frequently deadly illness known as primary amebic meningoencephalitis (PAM). Because of its thermophilic characteristics, N. fowleri is frequently found in freshwater that is warm habitats (Visvesvara et al., 2007a). PAM develops when N. fowleri is inadvertently introduced into the nose. The ameba then enters the central nervous system (CNS) through the olfactory nerves and cribriform plate. The consequences of a CNS invasion include cerebral edema, necrosis, herniation, and, most often, death. By examining the tissue of the brain or cerebrospinal fluid (CSF) under a microscope, it is possible to make an educated guess about the presence of N. fowleri infection (Visvesvara, 2010). PAM a hemorrhagic-necrotizing meningoencephalitis primarily affecting immunocompetent children and young adults, is brought on by N. fowleri. Summertime is the most common time for this illness to arise since people are swimming for fun and the water temperature is adjusted to meet the amoeba's thermal requirements (Bonilla-Lemus et al., 2020).
Seven to ten days after infection, the acute hemorrhagic necrotizing meningoencephalitis that accompanies CNS invasion usually leads in mortality (Martinez and Visvesvara, 1997).
6.Host Immune Responses to N. fowleri Infection
Water serves as a medium via which Naegleria fowleri enters the upper nasal mucosa. After there, it reaches the cribriform plate's sub-olfactory area, which is where the olfactory bulb is situated. As it ascends via this plate's pores and initially comes into contact with the tissues surrounding this particular area and the olfactory epithelium/bulb (Baig and Khan, 2014). The microscopic patterns that appear and the cytokines that are generated in PAM patients provide insight into the host immune response to Naegleria fowleri. The olfactory region's macrophages have a tendency to attract a high influx of neutrophils when infected with Naegleria fowleri. As demonstrated at autopsy, there is significant cerebral edema and neuronal tissue damage due to the acute inflammatory cytokines created by the local and recruited leukocytes, as well as the release of proteases, collagenase, and several other tissue-destructive lysosomal products by the inflammatory white blood cells (Baig, 2015). Leukocytes enter the neural tissue when the blood-brain barrier is disrupted, with neutrophils and macrophages making up the majority of these lesions. In PAM, complement activation, tissue-destructive cytokines, and the proteases generated by the Naegleria trophozoites induce cytotoxicity, resulting in the development of an offibrino-suppurative exudate-based lesion. Hemorrhage resulting from injury to the microvasculature is seen on both microscopic and large slides made from autopsied brains (Cerva, 1989).
7.Clinical and Laboratory Diagnosis
Although some cases have been documented within 24 hours of infection rate, clinical symptoms and indicators of N. fowleri infections often appear 2 to 8 days after infectivity (Visvesvara et al., 2007b). The most typical symptoms of an N. fowleri infection are photophobia, disorientation, seizures, severe headache, fever, chills, positive Brudzinski sign, positive Kernig sign, and maybe even coma. Specific signs and symptoms are not present. Furthermore, in few instances, myocardial necrosis and irregular heart rhythms have been noted (Grace et al., 2015a). The most significant finding is that higher intracranial pressure and cerebral spinal fluid (CSF) pressure have been linked to mortality. Patients infected with N. fowleri have been reported to have CSF pressures as high as 600 mm H2O. When examining a fresh sample of CSF under a microscope, the motile amebae are frequently observed moving quickly. Brain abnormalities are frequently visible on magnetic resonance imaging (MRI), which displays abnormalities in the midbrain and subarachnoid space, among other parts of the brain (Visvesvara et al., 2007b). To recognition, the amebae may be colored as well using a number of staining, including Giemsa-Wright or a modified trichrome stain (Visvesvara, 2010).
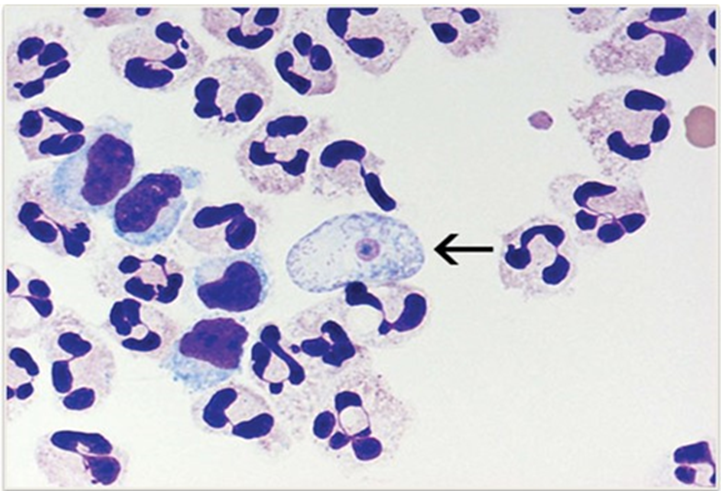
Figure 4: An N. fowleri trophozoite (arrow) stained with Giemsa-Wright is shown in a cytospin of fixed CSF surrounded by polymorphonuclear leukocytes and a few lymphocytes. One can observe the nucleus and nucleolus inside the trophozoite (Capewell et al., 2014)
8.Treatments
It is crucial to emphasize that selecting a suitable therapy depends on having a proper diagnosis. Nevertheless, most individuals infected with this bacterium pass away, and PAM is not frequently detected in the early stages of illness. There is an immediate need for additional effective medications due to the high death rate. Research on drug development has advanced since the initial PAM study (Rice et al., 2015). There are currently no clinical trials
evaluating the superiority of one treatment plan over another since N. fowleri infections in humans are uncommon. The majority of data pertaining to the effectiveness of medications is derived from either in vitro research or case reports. A number of case reports and in vitro studies have examined amphotericin B, which is arguably the most often prescribed drug for treating N. fowleri infections. The cornerstone of therapy is thought to be the polyene antifungal amphotericin B. It functions by attaching itself to ergosterol in the cell membrane to create holes that change the permeability of the membrane and cause the cell to die (Grace et al., 2015b).

Figure 5: specimen from a Caucasian 12-year-old girl. Naegleria fowleri on oil-immersed cytospin slides with cerebrospinal fluid (CSF) stained with Wright-Giemsa (original magnification, ×1000). Naegleria organisms are shown with arrows (Dunn et al., 2016)

Figure 6: Phase contrast microscopy image of a wet mount of Naegleria fowleri trophozoites grown from a patient's CSF for primary amebic meningoencephalitis (PAM) (Visvesvara et al., 2007a).
According to the current study, quinazolines by themselves or in combination with silver nanoparticles may be effective treatments for amoebae that feed on the brain(Mungroo et al., 2020).
.Successful therapeutic approaches against PAM
A number of experimental medications have been explored in vitro to successfully kill the protozoan within the host that it infects because of the seriousness and lethal nature of the PAM disease processes. Additionally, the treatment plan for people infected with this bacterium seems to revolve around intensive therapy and early diagnostics. It looks that the most popular medication regimen for PAM patients is a mix of amphotericin B, rifampicin, and antifungal medications. Despite the fact that giving these medications to patients does not guarantee their life, they are nevertheless regarded as the
main therapeutic approach used to treat PAM in a clinical environment (Yadav et al., 2013). Because of this, a number of investigational therapeutic medications have been utilized in addition to the traditional combination medication therapy that PAM patients are receiving. Among the most promising medications is miltefosine (Heggie and Küpper, 2017). Miltefosine has demonstrated effectiveness when combined with other therapeutic medications such amphotericin B, rifampicin, fluconazole, and chlorpromazine, both in vivo mouse models and in vitro investigations, despite the fact that the precise impact of the drug on Naegleria sp. has not been further investigated (Kim et al., 2008). The antirheumatic medication auranofin was tested in a different study using axenic cultures of pathogenic strains of Naegleria fowleri. It was discovered that the drug had an amoebicidal effect on the protozoan, which reduced the number of amoebas in the cultures. This effect was observed even after accounting for auranofin's effects on the integrity of the protozoan membrane and the organism's decreased metabolic activity (Peroutka-Bigus and Bellaire, 2019). When studied with Amphotericin B in vitro and in mouse models, corifungin has also been shown to be more effective than the latter medication. Corifungin primarily causes rupture of the organism's plasma and cytoplasmic membranes, which results in amoeba lysis. Furthermore, the FDA has authorized configurin as an orphan medication for the treatment of PAM (Debnath et al., 2012).
10.Prevention and Control
The World Health Organization (WHO) states that immunization is the greatest and most efficient method of disease prevention. As an alternative, one might employ additional preventative measures to ward off N. fowleri infection. The majority of PAM instances happen when people engage in certain activities in amoeba-infested waterways, such swimming pools or natural bodies of water. Pools and water parks should be chlorinated to avoid PAM since N. fowleri is vulnerable to chlorine and is destroyed at one part per million. To find out if N. fowleri is present in such waters, the South Australian High Commission's ameba-monitoring programme regularly measures total coliform counts and residual chlorine levels. Global implementation of comparable initiatives might stop new cases of N. fowleri infection. Although N. fowleri infection has also been linked to household water sources, medical equipment, and hygiene products, chlorine should also be used to sanitize these items (Visvesvara, 2013). Because Naegleria fowleri is a thermophilic amoeba, it multiplies in water at temperatures higher than thirty degrees Celsius. There are precautions that people who play water sports in warmer areas may take, such as staying out of freshwater bodies like lakes, rivers, and ponds, especially in the summer whenever the water is warmer. Because N. fowleri cannot live in chlorinated or salted water, these conditions greatly reduce the likelihood of N. fowleri infections. In an effort to prevent N. fowleri from getting into the nasal passages, people should refrain from leaping into bodies of water, splashing, and immersing their heads in it, if they cannot avoid watery activities. When engaging in such activities is unavoidable, people should use nose clips to reduce the likelihood that water that is contaminated may get inside their noses (Cogo et al., 2004). Local public health authorities should take N. fowleri amoebae into consideration and publish relevant warnings, especially during the hot summer months. It is advised to warn kids not to submerge their heads in dubious waters (Schuster and Visvesvara, 2004).
Primary meningoencephalitis (PAM) is caused by the opportunistic free-living amoeba Naegleria fowleri. Diffuse hemorrhagic necrotizing meningoencephalitis causes a fast start and fulminant course in the clinical course of a neurological illness caused by Naegleria. Granulomatous amebic encephalitis and PAM are two types of primary amebic meningoencephalitis. N. fowleri is the main cause of PAM in a patient in good condition that has previously had close contact with fresh water, particularly during the summer. The neuroepithelium and olfactory mucosa serve as the entrance points. Patients often pass away within 7 to 10 days after the beginning of symptoms. The incubation period is between 3 and 8 days, with an acute and quickly lethal outcome. While the patient's clinical manifestations and indicators were comparable to those previously documented, hydrocephalus had not been documented earlier. Moreover, this is the first record of PM with hydrocephalus that is communicative. The majority of PAM cases are frequently mislabeled as acute tubercular meningitis or bacterial meningitis. In this instance, the patient was first treated for bacterial meningitis; however, because he did not improve, PAM was discovered at a follow-up assessment (Movahedi et al., 2012). Naegleria is often spread by swimming or diving in contaminated water, but it can also be contracted from other sources, including tap water and the air. In rare instances, cases of the infection have been documented when the victim washed their face or breathed in airborne cysts. Out of the seven pediatric PAM cases, only two patients have previous records of contact (Singh et al., 1998). PAM's first clinical symptoms, which include headache, fever, nausea, and vomiting, followed by altered consciousness and seizures, are quite similar to those of acute bacterial meningitis. This is also one of the causes of the low reported incidence of the condition, as the majority of patients go miss-diagnosed. In addition to having a fever and headache, our patient did not exhibit any focused deficiencies in his nervous system. The trichome or giemsa stain is primarily used to detect the presence of trophozoites in the cerebrospinal fluid (CSF), which is necessary for the diagnosis of Naegleria fowleri. The other CSF analysis results, such as increased opening pressure, are not particularly PAM-specific (Chen et al., 2019).
In conclusion, PAM is an exceedingly rare and deadly infection, but due to improved diagnoses, a rising prevalence is now being documented in developing nations. The deadly parasite Naegleria fowleri is the cause of primary amoebic meningoencephalitis in humans, with a fatality rate of about 95%. It is widely distributed in nations with extremely hot summers. When a human comes into touch with contaminated water, the parasite causes the illness. The infection starts when the infectious stage "Trophozoites" enters the nasal tube, travels to the brain, infects the central nervous system, and ultimately results in death within three to seven days. Amphotericin B is one drug that can treat this deadly illness, but it still kills people. Ultimately, it is imperative to conduct further research on this parasite and explore strategies for managing it to safeguard the immune system. PAM should be taken into consideration for any patient with pyogenic meningitis who does not exhibit any bacteria by staining, antigen detection, or culture, despite its rarity and dismal prognosis. In these situations, CSF cytology of wet mount becomes required since early amphotericin therapy may increase survival. Since early treatment can significantly improve the prognosis of the condition, diagnostic staff members should be more aware of the need of carefully examining CSF wet preparation in order to diagnose Naegleria infections quickly.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
