
Case Report | DOI: https://doi.org/10.31579/2693-4779/066
1 Neurosurgery Department Ali Ait Idir Hospital Health Establishment, Algiers, Algeria
2 Neurosurgery Department, Mustapha Pacha University Hospital, Algiers, Algeria
*Corresponding Author: F. Bouchenaki. Neurosurgery Department Ali Ait Idir Hospital Health Establishment, Algiers, Algeria.
Citation: F. Bouchenaki, k. badache, N. Habchi, M S. Benachour, S. Bakhti. (2021) Caudal Regression Syndrome. Clinical Research and Clinical Trials. 4(3); DOI: 10.31579/2693-4779/066
Copyright: © 2021 F. Bouchenaki, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 September 2021 | Accepted: 24 September 2021 | Published: 29 September 2021
Keywords: caudal regression syndrome; agenesis of the coccygeal or lumbosacral vertebrae - attached lower marrow syndrome - lipomatous filum
Caudal Regression Syndrome (CRS) is a rare malformation syndrome associating to varying degrees agenesis of the coccygeal or lumbosacral vertebrae.This vertebral anomaly can therefore be reduced clinically to a simple coccygeal agenesis without any deficit or even lumbosacral agenesis accompanying a clinical picture with sphincter disorders associated or not with transit disorders and various deficits involving the lower limbs.This syndrome is accompanied by other orthopedic malformations such as shortening of the lower limbs, and / or gastrointestinal abnormalities, see also genitourinary as well as cardiovascular.Its incidence is 1 to 5 cases per 100,000 births.
Its precise cause has not yet been identified, but its relationship to maternal diabetes is well established.
We report in our study 5 patients with CRS from different clinics whose sphincter disorders were found in the foreground in all our patients and whose results vary according to the inaugural clinical picture. MRI made it possible to refine and confirm the diagnosis highlighting the congenital anomaly and the associated lesions.We have obtained 75% good results and 25% clinical stabilization; nor do we deplore any case of aggravation or death.
The interest is to suspect the diagnosis of CRS; document it at the start of the prenatal period and determine its severity and associated abnormalities in order to present options for patient management; because once the diagnosis is made, surgical treatment becomes imperative due to the formidable neurological sequelae compromising the functional prognosis.
Caudal regression syndrome (CRS) is a rare disorder first described by Geoffroy Saint-Hilaire and Hohl in 1852, and in 1964 Duhmel coined the term “caudal regression syndrome” [2-3].It affects between 0.1 and 0.25 pregnancies in 10,000, with a male-to-female ratio of 2.7 [1].-In a prenatal context, approximately 20% of cases of caudal regression syndrome are associated with type I or type II diabetes mellitus in the mother [5] and / or carrying a hydramnios [6].From an embryological point of view, it is believed that CRS is the result of defects in the induction of caudal elements in the embryo before the 28th day of gestation [7].The vertebral anomaly can vary from a simple coccygeal agenesis without any deficit to lumbosacral agenesis with sphincter and intestinal transit disorders associating motor damage affecting the lower limbs of varying severity corresponding to the spinal cord segments concerned.Orthopedic malformations associated with the type of shortening of the lower limbs, and gastrointestinal abnormalities with the type of anal imperforation are frequently revealed in the literature review [3].The diagnosis must be made in order to avoid the installation of complications that involve the functional prognosis, leaving definitive neurological sequelae and sometimes life-threatening [6].
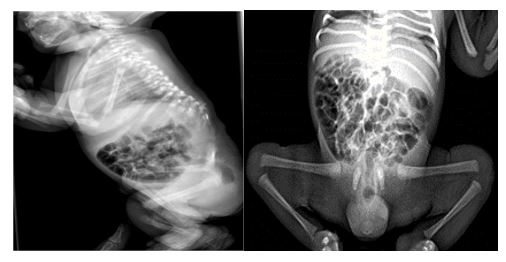
This is a retrospective study of 5 patients treated for caudal regression syndrome between January 2018 and May 2021.The average age was 3.5 years with extremes ranging from 08 months to 60 months. The reason for consultation was most often:-Sphincteric disorders are found in 4 patients, i.e. in 80% of cases.Represented mainly by:-Urinary tract infections which is a very common reason in these patients carrying this pathology,-Difficulty urinating- Transit disorders a type of obstinate constipation in 02 patients or in 40% of cases.-Motor sensory deficits which can go as far as complete cauda equina syndrome which was found in 01 case in the oldest child.-Orthopedic malformations:-A type of scoliosis in 03 cases.-Isolated deformities of club feet 02 cases with contractures of the lower limbs characteristic of sacral agenesis with narrow hips, hypoplastic gluteal muscles and a shallow intergluteal cleft are described in the literature.- Associated malformations can enrich the clinical picture and worsen the prognosis and will therefore require multidisciplinary management.-Anorectal malformations such as anal imperforation in 01 cases.-Gastro-intestinal abnormalities atresia of the duodenum trachea-esophageal fistulas 01 case -Congenital genitourinary abnormalities (renal agenesis or hydronephrosis) in 02 cases.-Imaging this is essential for the diagnosis, but also for the therapeutic decision.-Simple x-rays: Sacro-coccygeal agenesis is often associated with agenesis of the lumbar vertebrae as well as cone anomalies better explored by MRI.In caudal regression syndrome, Renshaw [11] classified agenesis into four types, in order of increasing severity:Type 1 (A): total or partial unilateral sacral agenesis.Type 2 (B): partial sacral agenesis. Usually a first sacral vertebra is normal or hypoplastic, the rest of the sacrum is absent.The malformation of the sacrum is bilateral and symmetrical.Type 3 and 4 (C and D): Agenesis variable at the lumbar level and total at the sacral level.The type of junction between the most caudal vertebra and the iliums determines whether the agenesis is type 3 or 4.



Prenatal ultrasound: Prenatal diagnosis is based on ultrasound The cone often ends well above the expected level sometimes even above L1. [7]The Sacrum may be absent or hypoplastic.The extremities of the fetus can be seen in a “cross-legged” or “Buddha” position.MRI is in general the following can be observed:- Agenesis of the lumbosacral or sacral vertebral body which is generally less than L1 and often limited to the sacrum. -the spinal cord with the distal tip to a blunt, blunt pointed end terminating above the expected level said the medullary cone has a wedge-shaped or cigar-shaped appearance. [8-9]Imaging can differentiate two large groups of patients with caudal regression syndrome. [12]Group 1: the medullary cone is blunt and ends above the normal level; sometimes there is an associated dilated central duct or cyst filled with cerebrospinal fluid at the lower end of the cone.Type 1 is associated with urinary and bladder dysfunction.A sacred motor deficit occurs, and corresponds to the level of vertebral agenesis while the sensitive functions are relatively preserved.



Group 2: The medullary cone is elongated and attached by a thickened terminal filum or intraspinal lipoma and ends below the normal level [5].Neurological disorders are more marked in this group.-Other associated nervous malformations described in the literature.

For the prognosis:
All our patients were operated on 2 patients stabilized and 3 patients improved.There are no cases of motor or sphincter aggravation.Treatment and prognosis depend on the extent of the regression because Morbidity mainly concerns genitourinary and neuromuscular complications and management options are often centered on these with both urological and orthopedic support.
Caudal regression syndrome covers a range of orthopedic, gastrointestinal, genitourinary and neurological congenital malformations.Its close relationship with maternal diabetes is well established, hence the importance of early prenatal diagnosis for adequate management.The doctor's role is to suspect CRS in a diabetic mother, hence the importance of an early prenatal diagnosis for adequate management and to document it at the start of the prenatal period and determine its severity as well as the associated anomalies. in order to present options to the patient.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
