
Research Article | DOI: https://doi.org/10.31579/2690-8794/102
1 M.Sc. Clinical Psychology, Dev Sanskriti University, Ranchi, India.
2 M.Phil Clinical Psychology, RINPAS Ranchi, India.
*Corresponding Author: Deepshikha Paliwal, M.Sc. Clinical Psychology, Dev Sanskriti University, Ranchi, India.
Citation: Deepshikha Paliwal and Anamika Rawlani (2022) Case Study of a Middle-Aged Woman’s OCD Treatment Using CBT and ERP Technique. Clinical Medical Reviews and Reports 4(3): DOI: 10.31579/2690-8794/102
Copyright: © 2022, Deepshikha Paliwal, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 September 2021 | Accepted: 04 December 2021 | Published: 10 January 2022
Keywords: OCD; CBT; ERP; salkovskis’s model
Introduction: This is a case report of a middle-aged woman, who was experiencing “obsessive” thoughts related to the “Bindi” (decorative piece wear by women on the forehead) and cleaning “compulsions”. Present case report discusses the patient’s assessment, case formulation, treatment plan and the effectiveness of the CBT and ERP sessions in reducing OCD symptoms.
Methodology: The patient was treated with Cognitive Behavior Therapy (CBT) along with Exposure Response Prevention (ERP) technique. The assessment of the case was done with the Y-BOCS rating scale, Beck’s Depression Inventory, Obsessive Beliefs Questionnaire, and Behavior Analysis Performa which suggested the higher severity level of the patient’s symptoms. Parallel to the assessment sessions, detailed case history related to the onset of the problem, difficulties faced because of the disorder, childhood incidences, family chart, marital issues, and medical history were discussed with the patient. Based on the reported details, the case was formulated according to the Salkovoskis inflated sense of responsibility model. After the case formulation, the treatment plan was designed which involved ERP sessions and restructuring of the cognitive distortions (beliefs, thoughts, and attitude).
Results: After the completion of the twenty-five therapy sessions, the patient reported improvement in the coping of anxiety-provoking thoughts and reduced level of the washing compulsions. The effects of the therapy were checked and found maintained up to two months follow up.
Conclusion: CBT and ERP technique is an effective treatment in reducing obsessive and compulsive symptoms of the patient.
Have you ever felt like a sudden urge to hurt somebody? What if such urges continuously appear in your head? What would you do to stop these urges? Would you be able to continue your day to day life normally with such urges? Clinical Psychologists studied the repetitive occurrence of unwelcoming thoughts, urges, doubts, and images which create anxiety. They gave it the term “Obsessions”. These obsessions are dreadful, frightening, and intolerable to the extent that they might hinder the natural flow of one’s personal, professional, and social life. The person who suffers from such anxiety-provoking thoughts tries to deal with the distress caused by such ‘obsessions’ by adopting some behavior or activity which temporarily relieve them from the anxiety and the feared consequences. This behavior could be anything like washing hands, cleaning, repeatedly checking the door, or repeating some phrases in the head. Psychologists called such repetitive behaviors or activities as “Compulsions”. According to APA (1994), if the presence of obsessions and/or compulsions is time-consuming (more than an hour a day), cause major distress, and impair work, social, or other important functions then the person will be diagnosed with Obsessive-Compulsive Disorder (OCD). Recent epidemiological studies suggest that OCD affects between 1.9 to 2.5% of the world population at some point in their lives, creating great difficulties on a professional, academic and social level (DSM-IV-TR, 2001). OCD affects all cultural and ethnic groups and, unlike many related disorders, males and females are equally affected by this disorder (Rasmussen & Eisen, 1992). OCD is one of the most incapacitating of anxiety disorders having been rated as a leading cause of disability by the World Health Organization (1996). The major cause of OCD is still unknown; there could be some genetic components responsible for it (DSM-5). Child abuse or any stress-inducing event could be the risk factor involved in the history of OCD patients. The severity of the symptoms related to obsessions and compulsions provides the basis of the diagnosis in OCD which rules out any other drug-related or medical causes. Clinical Psychologists use rating scales like Y-BOCS (Fenske & Schwenk, 2009), self-reports, and Behavior Analysis Performa to assess the severity level of the symptoms. Based on the severity, the treatment plan is designed. Treatment of OCD involves psychotherapy and antidepressants. Psychotherapy such as Cognitive Behavior Therapy (CBT) is an effective psycho-social treatment of OCD (Beck, 2011). In CBT, a “problem-focused” approach is used to treat the diagnosed psychological disorder by challenging and changing core beliefs, negative automatic thoughts, and cognitive distortions of the patient. CBT involves Exposure Response Prevention (ERP) as a technique to treat OCD in which the patient is exposed to the cause of the problem and not allowed to repeat the ritual behavior (Grant, 2014). ERP has promising results with 63% of OCD patients showing favorable responses after following the therapy sessions (Stanley & Turner, 1995).
This is a case of a 31 years old woman, who belongs to a middle socio-economic background, currently living with her in-laws, husband, and daughter. The patient was experiencing obsessive thoughts related to the contamination spread by ‘bindi’ along with the compulsive behavior of washing and cleaning from the last five years. The patient reported that she always tried to check the contact of ‘Bindi’ with anything because that contact makes her incapacitate to control the situation. She took two and three hours (on daily basis) in washing and cleaning her home, scrubbing her daughter, cleaning the daughter’s school bag after returning from school, husband’s bag, and other usable items, so that she can stop the contamination from spreading everywhere. The patient has a history of facing interpersonal issues with family members since her childhood. Her father was alcohol dependent and the mother was the patient of depression. The financial condition of the family was not good. When the patient was 17 years old, her father died due to kidney failure, and her mother got hospitalized because of depression. From a very young age, the patient had to bear the responsibility of the family by taking tuitions. At first, she developed the fear of contamination at the age of 19, when she was in her graduation’s first year, for that she was taken to the Psychiatrist. She responded well to the medicines and stopped showing all the symptoms. At the age of 25, when the patient got pregnant she again developed the fear of contamination, which made her husband and in-laws uncomfortable and family disputes began. Her husband took her to the psychiatrist who referred her for the psychotherapy but she didn’t attend the psychotherapy sessions properly and continuously lived with the obsessions and compulsions up to the present referral where the patient was assessed with Y-BOCS rating scale, BDI, EBQ, and Behavioral Analysis Performa. Based on the assessment, she was diagnosed with OCD having symptoms of obsessions related to the contamination by ‘Bindi’ and washing compulsions. Detailed case history related to the onset of the problem, childhood incidences, family history, marital history, medical history, and other relevant information were also collected. The case was formulated according to Salkovoskis’s inflated sense of responsibility model as the patient’s reported details were signifying the negative interpretations of her responsibility for self and others. After the case formulation, the treatment plan was designed which involved sessions of ERP technique along with the alteration of cognitive distortions (ideas, beliefs, and attitudes) through the cognitive restructuring method of CBT.
Measures
1. Yale-Brown Obsessive-Compulsive Scale (YBOCS):
In cognitive-behavioral studies, Y-BOCS is used to rate the symptoms of OCD. This scale was designed by Goodman et al. (1989) to know the baseline and the recovery rate of the ‘severity of obsessions’, ‘severity of compulsions’ and ‘resistance to symptoms’. This is a five-point Likert scale that clinicians administer through a semi-structured interview in which a higher score indicates higher disturbances. The excellent psychometric properties of this scale quantify the severity of the obsessions and compulsions as well as provide valuable qualitative information which makes it very useful for both diagnosis of the OCD and the designing of its treatment plan.
2. Beck Anxiety Inventory (BAI):
Aaron T. Beck (1988) developed BAI as a four-point Likert scale which consists of 21 items of ‘0 to 3’ scores on each item (Higher score means higher anxiety). If the Patient’s scores are from 0 to 7 then interpret as ‘minimal anxiety’, 8 to 15 as ‘mild anxiety’, 16 to 25 as ‘moderate anxiety’, and 30 to 63 as ‘severe anxiety’. BAI assesses common cognitive and somatic symptoms of anxiety disorder and is considered effective in discriminating between the person with or without an anxiety disorder. This scale provides valuable clinical information but is not used by clinicians for diagnostic purposes.
3. Obsessive Belief Questionnaire (OBQ):
OBQ is used to assess the beliefs and appraisals of OCD patients which are critical to their pathogenesis of obsessions (OCCWG, 1997, 2001). This scale consists of 87 belief statements within six subscales which represent key belief domains of OCD. The first subscale is ‘Control of thoughts’ (14 items), the second is ‘importance of thoughts’ (14 items), third is, responsibility (16 items), fourth is ‘intolerance of uncertainty’ (13 items), the fifth is an overestimation of threat (14 items), and sixth is ‘perfectionism’ (16 items). Response on this measure is the general level of agreement of the respondents with the items on a 7 point rating scale that ranges from (-3) “disagree very much” to (+3) “agree very much”. On the respective items summing of the scores is done to calculate the subscale scores.
4. Behavior Analysis Performa
This study used ‘Behavior Analysis Performa’ to do the functional analysis of the patient’s behavior. This Performa collects the details of the patient’s behavioral excess, deficits, and assets, his or her motivational factors behind maintaining and reinforcing ill behaviors, as well as, the medical, cultural, and social factors which contributed to the development of the illness.
Based on the reported details and the assessment, the case was formulated according to the Salkovoskis model (1985). This model suggests that the patient’s main negative interpretation revolves around the idea that his or her actions might have harmful outcomes for self or others. This interpretation of responsibility increases selective attention and maintains negative beliefs (Salkovskis, 1987). Here, in this case, the patient had to face the disturbing family environment which significantly has a role in the formation of maladaptive schemas related to her negative view of self, the world, and the future. The patient’s beliefs assessment reports signified that her major dysfunctional assumptions were ‘if harm is very unlikely, I should try to prevent it at any cost’ and ‘if I don’t act when I foresee danger then I am to blame for any consequences’. Intrusive thought for her was that ‘bindi contaminates dirt’ and neutralizing action for this intrusive thought was ‘washing and cleaning things’. She paid her keen attention to the thought that ‘I should not be get touched with bindi’ and misinterpreted and over signified it by avoiding bindi and preventing the contamination. Her safety behavior included avoiding going out, (especially beauty parlors and cosmetic shops), and getting touched with anyone on roads and market places. The result of such avoidance was tiredness, anxiousness, aggressiveness, and distressed mood state. The graphical representation of the case formulation is shown in Appendix 1 at the end of this paper.
After the case formulation, the treatment plan was designed. The patient had dysfunctional assumptions related to her responsibility for self and others. She had obsessions related to the contamination spread by ‘Bindi’ associated with washing and cleaning compulsions. As she was taken by her husband for the therapy, so it was important to socialize her and her family with the OCD to develop insight for the disorder. After socializing them with OCD, they were taught the basic structure of the cognitive behavior model that how patient’s thoughts, emotions, physical sensations, and behavior all are interrelated and affect each other in a vicious circle.
In the preparatory phase, the patient was introduced with the ERP technique, how does it work and how much her cooperation and will power are required for the success of this technique. After introducing the ERP technique to her, behavioral analysis was done with the patient by using a down-arrow method to make the list of the situations she uses as safety strategies and maintains her negative beliefs.
In the next session, the patient was told to imagine her exposure with different situations which she avoids and asked her to rate the level of anxiety in all the situations on a scale of 1 to 10. After this imaginary exposure, a hierarchy was made from the least anxiety-provoking event to the high anxiety-provoking event. Here is the list of different situations which the patient rated based on the level of anxiety:
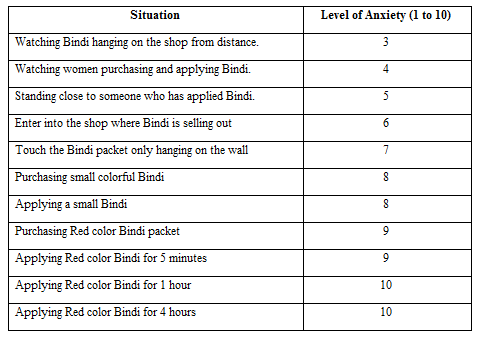
In this phase, the patient was gradually exposed with the least anxiety-provoking situation to the highest-anxiety provoking situation. The patient’s husband worked as a co-therapist and accompanied her in all the situations and observed her anxiety levels and other behaviors. The patient was asked to rate her anxiety level on a scale of 1 to 10 after every exposure.
With each ERP session, the patient came to realize that the nature of anxiety is that it goes up with the triggering event but with the passage of time, automatically comes down. She also developed the insight that she had fear from the thoughts of contamination and with its associated anxiety more than ‘Bindi’ itself.
After the ERP sessions, the patient was given two booster sessions in which she was taught the ways to deal with the anxiety after the termination of therapy in her day to day life situations. In those sessions, she was asked to imagine her home, her room, and herself with Bindi on her forehead and doing household chores like cooking, cleaning the things, etc. When the patient was asked to express herself during the imagination, she reported that she is feeling more confident now to stick on her thought that bindi can’t contaminate, it’s her idea and there is no use of washing hands and other things because of the fear of contamination. Her husband and mother-in-law were also instructed to remind her again and again about the things she learned during the therapy sessions. After the declaration of the patient that she is feeling better now and ready to face the anxiety on her own, therapy sessions were terminated.
Follow up:
One month later, the patient was contacted for the follow-up and asked about her coping with the anxiety through telephonic conversation. She reported that thoughts of contamination came in her mind but she is in better condition than previous after taking the ERP sessions.
After two months, the patient came for the session again with the complaints that sometimes she became weak and washed her hands with the thought of contamination. After washing, she repented on her behavior which lowers down her confidence in conquering over the illness. Then she was instructed that washing hands strengthens the thought of contamination so she should avoid it as much as possible but this doesn’t mean that she has not gained anything with the therapy, she was reminded about her previous condition that how much it was unbearable for her to even think about the bindi but now she is applying it on her forehead which shows that only the traces of the illness left, most of it is already recovered. In this way, the patient became relaxed and felt more determined to continue with the learnings during the sessions.
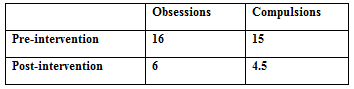
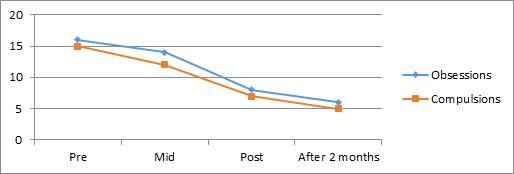
After the termination of the therapy sessions, the patient’s obsessive and compulsive symptoms were found reduced on the Y-BOCS symptom checklist:
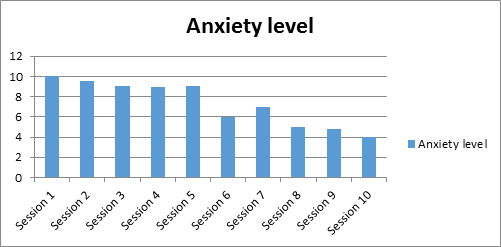
With the graded exposure sessions, her anxiety level also came down from the rating of 10 in the beginning sessions to the rating of 4 in the endings sessions on a scale of 1 to 10.
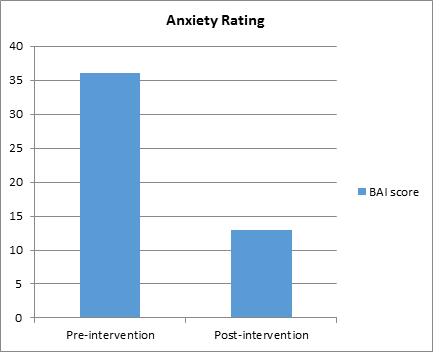
The patient’s BAI score was also fallen down from pre-intervention- 36 (Extreme level of anxiety) to post intervention-13 (mild level of anxiety) which suggests 36% reduction in the anxiety level of the patient.
Previous research findings considered CBT as the most promising treatment of OCD (Stanley & Turner, 1995; Foa et al, 1999). CBT emphasizes the integration of cognitive-behavioral strategies like discussion techniques (Guided Discovery) and behavioral experiments (ERP) to formulate the problem and direct the treatment. Therapists try to identify the key distorted beliefs along with patients and allow them to test their beliefs which develop and maintain compulsive behaviors. This case identified the contamination with ‘Bindi’ as the pathological belief which was maintaining the compulsive behaviors of washing and cleaning. The cognitive hypothesis of Salkovoskis (1985) proposed that the origin of obsessional thinking lies in normal intrusive ideas, images, thoughts, and impulses which a person finds unacceptable, upsetting, or unpleasant. The occurrence and content of these intrusive cognitions are negatively interpreted as an indication that the person may be ‘responsible for harm’ or ‘prevent the harm’. Such an interpretation is likely followed by emotional reactions such as anxiety or depression. These emotional reactions lead to discomfort and neutralizing (Compulsive) behaviors like washing, cleaning, checking, avoidance of situations related to the obsessive thought, seeking reassurance, and attempts to exclude these thoughts from the mind. The present case supported this hypothesis of Salkovoskis’s model as intrusive thought of the patient was contamination spread by ‘Bindi’ which negatively interpreted as ‘I can avoid the likely harms by avoiding the contamination spread by Bindi’, such negative interpretation was raising her anxiety levels, making her attentive selective towards the ‘Bindi’, maintaining her compulsive acts and complying her to adopt the safety strategies.
Rachman (1983) predicted that behavioral experiments, in which the patient is exposed to the feared object, these intrusive thoughts are challenged by changing the pattern of thinking and behaving. Hodgson & Rachman (1972) initiated the series of clinical studies on patients with contamination and predicted that immediate washing reduces the anxiety. In one of their experimental study, they noted a similar degree of anxiety reduction when the patient was asked not to perform a compulsive act for one hour. They termed this phenomenon as ‘spontaneous decay’ which was established as the basis of ERP. Also, Foa & Kozak (1986) proposed that exposure techniques activate the network of cognitive fear and patients get new experience which is different from the existing pathological beliefs. This case confirmed this hypothesis as the patient initially thought that her exposure with ‘Bindi’ might cause some uncertain consequence with her but prolonged exposures provided her new experience that she could manage with her fear and anxiety which resulted in the improved coping with obsessional beliefs about contamination and urge to wash and clean. Her improved coping is evident in the statistically significant reduction of her scores on the standard measures like the Y-BOCS symptom checklist, BAI, and OBQ.
The results of this case study add on the value of CBT (that involves ERP technique) in the treatment of obsessive thinking related to the ‘fear of contamination’ and compulsive behavior of ‘washing and cleaning’. However, there is a need for more such case studies with more precision and effective treatment designs to provide valuable information related to the nature of OCD and its treatment.
In this case of OCD, patient’s symptoms were reduced to a manageable level and found maintained for two months which provides an evidence of the effectiveness of CBT and ERP technique in the treatment of OCD.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
