
Case Report | DOI: https://doi.org/10.31579/2641-0419/007
1 Internal Medicine Department, Max Super Specialty Hospital. Saket, India.
*Corresponding Author: Swati Kapoor, Internal Medicine Department, Max Super Specialty Hospital. Saket, India.
Citation: Neeraj Awasthy, Swati Kapoor, Rajeev Upreti , Kulbhushan Dagar, Situs Inversus With Dextrocardia And Transposition Of Great Arteries From Diagnosis To Management. J. Clinical Cardiology and Cardiovascular Interventions. 1(2); DOI:10.31579/2641-0419/007
Copyright: © 2018. Swati Kapoor. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 May 2021 | Accepted: 29 May 2018 | Published: 06 June 2018
Keywords: balloon atrial septostomy, fogarty embolectomy catheter, atrial switch surgery
Situs inversus totalis is a rare anomaly. A 40 day old girl presented to our emergency with this condition. She also had intact ventricular septum and D-transposition of the great arteries. Balloon atrial septostomy is usually a lifesaving procedure in such patients, till the corrective surgery is performed. In our case, this procedure was performed in the patient and we discuss the implication of her abnormal anatomy in the ease of management of this case. To our knowledge, this is the first case report of such a procedure in a patient with this unusual presentation.
The position of the atria of heart and other viscera of body describes the ‘situs’, situs solitus being the normal position and situs inversus is the mirror image of situs solitus-the morphological right atrium is on the left and the morphological left atrium is on the right. When situs inversus is present along with dextrocardia, it is termed as situs inversus totalis. It is a rare condition with a prevalence of 1:10,000 in some populations1. In this condition, major visceral organs are also a mirror image of the normal2. Five to ten percent of these patients also have congenital heart defects, of which transposition of great arteries (TGA) is the most common. Though the management of TGA involves corrective surgery, an atrialse ptostomy done early in time is lifesaving.
A 2.9 kg term girl child delivered by spontaneous delivery with Apgar scores of 9 and 9 at 1 and 5 minutes was evaluated for bluish discoloration at birth. On physical examination child was cyanosed with baseline oxygen saturation of 55 % with respiratory distress with respiratory rates of 75 /minute and subcoastal retractions. He had normal precordium on palpation with normal 1st heart sound and a single loud 2nd heart sound. The liver was palpable 3 cm below the left costal margin.
Chest radiography demonstrated dextrocardia, cardiomegaly (cardiothoracic ratio >0.6), a right aortic arch, and clear lung fields with normal pulmonary vascularity(Figure 1).
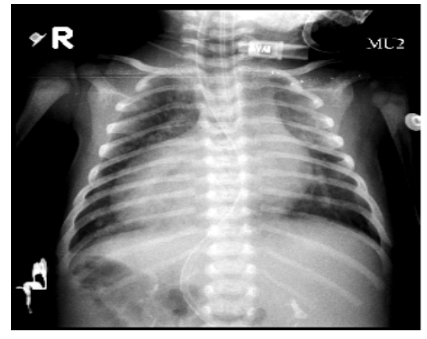
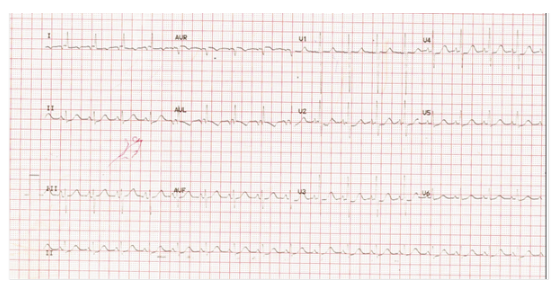
A gastric air bubble was noted on the right side, and a liver shadow was visible on the left side. The electrocardiogram revealed a low left atrial rhythm and dextrocardia (Figure 2). Abdominal ultrasound demonstrated the stomach and spleen on the right side and the liver on the left. The aorta and the inferior vena cava were inverted. Echocardiography demonstrated dextrocardia, abdominal and atrial situs inversus, atrioventricular concordance, and ventriculo-arterial discordance with l-posed aorta, tricuspid aortic and pulmonary valve and there was mild pulmonary regurgitation, laminar flow in left and right ventricular outflow tract with tiny interatrial communication (1.5mm). Interventricular septum was intact and there was left-to-right shunting through a patent foramen ovale with mean pulmonary gradient of 5 mm hg. There was tiny closing patent ductus arteriosus with right aortic arch.
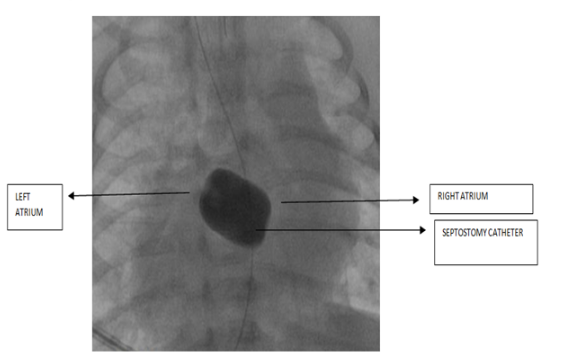
Her initial blood gas report was suggestive of metabolic acidosis (pH of 7.08, with base deficit of –12).The patient was electively intubated and a prostaglandin infusion was initiated. Child underwent balloon atrial septostomy to improve mixing at the atrial level. Septostomy was carried under echocardiography and fluoroscopy guidance using Fogarty 4 French (Edwards Laboratories, Santa Ana, California, United States of America) embolectomy catheter. Unusual anatomy of the atrial septal plane facilitated easy entry from the right atrium to left atrium with minimal modulation of the angulation of the catheter. Oxygen saturation improved to 85% in room air following the procedure, and the prostaglandin was discontinued.
On 41st day of life, the patient underwent arterial switch operation. Under full-flow cardiopulmonary bypass, the aorta and pulmonary arteries were transected, a Lecompte maneuver was performed, and the coronary arteries were re-anastomosed to the aorta in the standard fashion. The atrial and ventricular septal defects were patched using a transatrial approach (Figure 3 and figure 4).

Postoperative transesophageal echocardiography demonstrated no new obstruction in the aorta or pulmonary artery, and no residual shunting at the atrial or ventricular level. She had an uneventful postoperative course, and was extubated within 94 hours and weaned from hemodynamic support by 5th postoperative day and discharged by 10 postopertaive day with normal echo at discharge.
Situs inversus totalis is a rare condition with a prevalence of 1:10,000 in some populations1. About 5 to 10 % of patients with this defect also have congenital heart defects. These defects are varied. D-TGA is the most common congenital heart lesion which affects about 2.6 to 7.8% of these patients3. Though the management of TGA involves corrective surgery for this congenital defect, creation of an interatrial communication via a balloon or blade atrial septostomy allows the mixing of the oxygenated blood at the atrial level and is lifesaving4. The corrective surgery is usually done at a later date.
The usual procedure involved for atrial septostomy involves introducing the septostomy catheter from the inferior vena cava to right atrium, to create an interatrial communication between the right and left atria, so that there is intermixing of oxygenated and deoxygenated blood through this communication. This intermixing is vital for the newborn baby born with TGA to survive.
In our reported case, successful balloon atrial septostomy (BAS) followed by neonatal arterial switch was performed in a patient with atrial and visceral situs inversus totalis, atrioventricular concordance, and ventriculo-arterial discordance. The fact that the patient had unusual anatomy of the atrial septal plane facilitated easy entry from the right atrium to left atrium. The presence of situs inversus totalis oriented the interatrial septum in a suitable way to facilitate the entry of septostomy catheter from right atrium to left atrium. Normally the septostomy catheter requires an angulation (distally) to facilitate it’s entry from right atrium to left atrium. In the present case, the orientation of the interatrial septum was such that the angulation required was minimal.
Though abnormal, but this anatomy of our patient was in fact suitable for performing the BAS procedure. Even after extensive search, we were not able to find any such procedure reported in literature till now. This case report seems to be the first report of BAS operation in a patient with such abnormal anatomy.
The position of the atria of heart and other viscera of body describes the ‘situs’, situs solitus being the normal position and situs inversus is the mirror image of situs solitus-the morphological right atrium is on the left and the morphological left atrium is on the right. When situs inversus is present along with dextrocardia, it is termed as situs inversus totalis. It is a rare condition with a prevalence of 1:10,000 in some populations1. In this condition, major visceral organs are also a mirror image of the normal2. Five to ten percent of these patients also have congenital heart defects, of which transposition of great arteries (TGA) is the most common. Though the management of TGA involves corrective surgery, an atrialse ptostomy done early in time is lifesaving.
A 2.9 kg term girl child delivered by spontaneous delivery with Apgar scores of 9 and 9 at 1 and 5 minutes was evaluated for bluish discoloration at birth. On physical examination child was cyanosed with baseline oxygen saturation of 55 % with respiratory distress with respiratory rates of 75 /minute and subcoastal retractions. He had normal precordium on palpation with normal 1st heart sound and a single loud 2nd heart sound. The liver was palpable 3 cm below the left costal margin.
Chest radiography demonstrated dextrocardia, cardiomegaly (cardiothoracic ratio >0.6), a right aortic arch, and clear lung fields with normal pulmonary vascularity(Figure 1).
Situs inversus totalis is a rare condition with a prevalence of 1:10,000 in some populations1. About 5 to 10 % of patients with this defect also have congenital heart defects. These defects are varied. D-TGA is the most common congenital heart lesion which affects about 2.6 to 7.8% of these patients3. Though the management of TGA involves corrective surgery for this congenital defect, creation of an interatrial communication via a balloon or blade atrial septostomy allows the mixing of the oxygenated blood at the atrial level and is lifesaving4. The corrective surgery is usually done at a later date.
The usual procedure involved for atrial septostomy involves introducing the septostomy catheter from the inferior vena cava to right atrium, to create an interatrial communication between the right and left atria, so that there is intermixing of oxygenated and deoxygenated blood through this communication. This intermixing is vital for the newborn baby born with TGA to survive.
In our reported case, successful balloon atrial septostomy (BAS) followed by neonatal arterial switch was performed in a patient with atrial and visceral situs inversus totalis, atrioventricular concordance, and ventriculo-arterial discordance. The fact that the patient had unusual anatomy of the atrial septal plane facilitated easy entry from the right atrium to left atrium. The presence of situs inversus totalis oriented the interatrial septum in a suitable way to facilitate the entry of septostomy catheter from right atrium to left atrium. Normally the septostomy catheter requires an angulation (distally) to facilitate it’s entry from right atrium to left atrium. In the present case, the orientation of the interatrial septum was such that the angulation required was minimal.
Though abnormal, but this anatomy of our patient was in fact suitable for performing the BAS procedure. Even after extensive search, we were not able to find any such procedure reported in literature till now. This case report seems to be the first report of BAS operation in a patient with such abnormal anatomy.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
