
Case Report | DOI: https://doi.org/10.31579/2768-2757/055
1 General Surgery Resident, Oman Medical Specialty Board, Muscat, Oman.
2 Consultant Breast Surgery, Royal Hospital, Muscat, Oman.
*Corresponding Author: Tamadher Al Barhi, General Surgery Resident, Oman Medical Speciality Board, Muscat, Oman.
Citation: Tamadher Al Barhi, Matar Al Badi, Ibrahim Al Waili. (2022). Case Report: Unusual Volvulus with Internal Herniation Through a Defect in the Small Bowel Mesentery. Journal of Clinical Surgery and Research, 3(5); DOI:10.31579/2768-2757/055
Copyright: © 2022 Tamadher Al Barhi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 June 2022 | Accepted: 23 June 2022 | Published: 29 June 2022
Keywords: flexible ureteroscope; holmium laser; endogenous renal cyst; kidney calculi; curative effect analysis
Internal hernia is a surgical pathology that is caused by protrusion of intra-abdominal viscus through an aperture in the peritoneum of the mesentery. This defect can be congenital or acquired. Although it is rare, it can cause 0.6-5.8 % of small bowel obstruction. Patients with internal hernia complications can be missed as simple bowel obstruction where the management is almost different. In this paper, we are presenting a patient who came to our hospital with small and large bowel obstruction, eventually found to have an internal hernia due to a defect in the mesentery. Eventually required reduction of the hernia and resection of the diseased bowel.
Internal hernia (IH) is a protrusion of intra-abdominal viscus, usually the small bowel, through an aperture in the peritoneum or the mesentery within the abdomen or the pelvis [1]. Internal hernia can be congenital like paraduodenal and pericecal or acquired like post-surgery or due to a blunt abdominal trauma. Herniation through the omentum in a virgin abdomen is rare but has been reported in some case series due to congenital omental defect [2]. Although IH is rare, it causes 0.6–5.8% of small bowel obstruction [1]. Due to growing of the surgical procedures like gastric bypass for bariatric management and liver transplantation, the incidence of internal hernia has increased recently [1]. IHs can remain silent for many years if easily reducible, but they can present with mild gastrointestinal symptoms or even acute abdomen with high mortality rate [1]. Herniation of the small bowel together with the sigmoid colon is an unusual event and can cause a fatal closed loop obstruction. Some patients have been managed with colonoscopic decompression for an impression of simple sigmoid volvulus, however, they do not improve, and after careful evaluation with computed tomography (CT scan), the definitive diagnosis of internal hernia is found and the management is changed to be surgical. Thus, careful investigation should be carried out before a management is initiated [3]. We present our experience with an adult male patient who presented with internal hernia due to a congenital mesenteric defect with concomitant small and large bowel obstruction which both required resection.
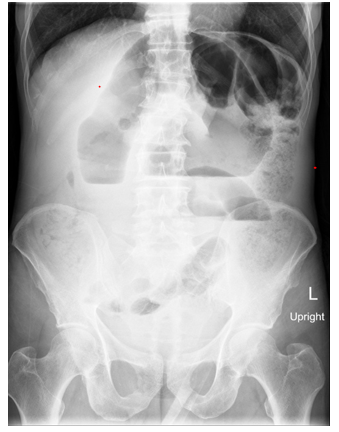
A previously healthy 62 years old smoker male patient presented to our emergency department for the first time in September 2020 complaining of lower abdominal pain. At that time, he was hemodynamically normal and his abdominal pain was mild. An abdominal x-ray was done which showed dilated small bowel loops with impacted stool, however there were no features suggestive of bowel obstruction or perforation [Figure1]. He was referred to surgical team for further review but the patient felt better and left the hospital before the surgical team arrive. He came back again in April 2021 complaining of bleeding hemorrhoids which were grade 2. He was discharged on conservative management and given a follow up appointment in the surgical out-patient department. Then the patient disappeared from the hospital until he showed up to the emergency department in March 2022 complaining of perianal pain as well as abdominal pain. Upon clinical assessment, he was hemodynamically normal, there was a non-complicated grade 3 hemorrhoid which was possible to be reduced manually. Regarding his abdominal pain which started the prior day, it was diffuse and not associated with nausea, vomiting, fever nor changes in bowel habit, which is constipation for him. Clinical examination showed a heart rate of 112, blood pressure 112/81 and a soft abdomen with mild diffuse tenderness. Initial laboratory investigations were as follow: hemoglobin of 15.4 g/dL, white blood cell count 9.9x10^9/L, neutrophils 8.8x10^9/L, platelet count 328x10^9/L, c-reactive protein <4>90 mL/min/1.73m2, Creatinine 66, normal liver function tests. Abdominal x-ray showed dilated bowel loops with air-fluid level with impacted stool in the colon [Figure 2], thus the patient was discharged on laxatives and analgesia, and was advised to report back to the hospital if his symptoms worsen or do not improve. Within less than 24 hours, he came back with worsening abdominal pain. On clinical assessment the patient was crying in pain, his temperature was 36.7, heart rate was 125, blood pressure 98/55 and respiratory rate of 40 breath/minute. His abdomen was distended, tense, tympanic on percussion and tender all over. Initial blood investigations showed hemoglobin 13.8 g/dL, white blood cell count 10.6x10^9/L, neutrophils count 7.7x10^9/L, platelet count 278x10^9/L, c reactive protein 100 mg/L, pH 7.18, Lactate 10.7 mmol/L, eGFR 24 mL/min/1.73m2, Creatinine 251, normal liver function tests. The patient was resuscitated immediately with IV fluid boluses, analgesia and broad-spectrum antibiotic (Tazocin). A Foley’s catheter inserted, however there was no urine output. Abdominal x-ray showed coffee bean sign which is suggestive of sigmoid volvulus [Figure 3]. The initial plan was to get a CT scan to further assess the pathology but because of the acute kidney injury and the patient’s critical status, this was canceled and the patient was taken for exploratory laparotomy after receiving the required resuscitation. Intra operatively, there was a sigmoid volvulus which was herniating together with a part of small bowel through a defect in the small bowel mesentery [Figure 4, 5]. The sigmoid colon and the herniated small bowel were gangrenous [Figure 6]. There was free hemorrhagic peritoneal fluid as well. The hernia was reduced and the gangrenous colon and small bowel were resected. Anastomosis was re-established by side-to-side anastomosis using a GIA stapler. Post operatively, the patient was monitored in an intensive care unit bed for 24 hours then shifted to a normal bed. He was kept nil per mouth and was on IV fluids as well as antibiotics and analgesia together with physiotherapy. On day 3 post operatively, bowel function started and diet was resumed slowly. He was discharged on day 7 post operatively in a good clinical health. The patient was seen in the surgical outpatient department and he was doing well.





Although internal hernia is a rare cause of intestinal obstruction, it carries high mortality rates when it happens. There are around 8 types of internal hernia including: para-duodenal 53%, peri-cecal 13%, foramen of winslow 8%, trans-mesenteric 35%, inter-sigmoid 6%, supra-vesical 6%, retro-anastomotic 5% and trans-omental 1-4% [4]. In adult patients, the incidence of acquired internal hernia is higher than congenital internal hernia with hernia through foramen of winslow being the most common, followed by trans-mesenteric hernia [4]. A defect in the mesentery can be congenital and usually present in children but can present at any age. In our patient, there was no risk factor for him to have a mesenteric defect, so a congenital mesenteric defect is the most likely possible etiology. Interestingly, his presentation a year ago with abdominal pain could be also explained by an internal hernia through the same mesenteric defect but have reduced spontaneously after receiving hydration and analgesia. The presentation of IH varies from vague abdominal discomfort to severe abdominal pain and tenderness. The diagnosis cannot be made easily with the clinical assessment or by the regular x-ray modality only. And although, CT scan is the gold standard technique to diagnose IH with 76% specificity and 63% sensitivity, it is still difficult to make the diagnosis [5]. In our patient, it was not feasible to get a CT scan as he was not hemodynamically stable enough to wait for the CT scan knowing that he will eventually require a surgical management for his bowel obstruction giving his abdominal examination findings and the high lactate level. Also, his deranged kidney function opted against waiting for a CT scan. IH management requires urgent reduction of the herniated segments with careful handling of the bowel to avoid iatrogenic injuries. The bowel should be assessed for viability, otherwise resection should be done.
Internal hernia although is rare but can present with small and large bowel obstruction. The most common type of internal hernia is hernia through the foramen of winslow, followed by trans-mesenteric defect. Careful diagnosis should be made with a CT scan if feasible as IH can be missed as a simple bowel obstruction. IH can reduce spontaneously, however, a surgical management is usually required to treat the primary etiology.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
