
Case Report | DOI: https://doi.org/10.31579/2690-8808/155
1 Founder and Medical Director- Institute of Minimally Invasive Thoracic Surgery, Hospital Angeles Lomas, Mexico City, Mexico. Vialidad de la Barranca 240, Hacienda de las Palmas, Huixquilucan, Estado de México 52763. 5521078324.
2 Department of General Surgery, Hospital Angeles Lomas, Mexico City, Mexico
3 Doctor of medicine and Medical Assistant- Institute of Minimally Invasive Thoracic Surgery, Hospital Angeles Lomas, Mexico City, Mexico
*Corresponding Author: Jose Manuel Mier Ordionzola, Founder and Medical Director- Institute of Minimally Invasive Thoracic Surgery, Hospital Angeles Lomas, Mexico City, Mexico. Vialidad de la Barranca 240, Hacienda de las Palmas, Huixquilucan, Estado de México 52763. 5521078324
Citation: Jose Manuel Mier Ordionzola, Atl Simon Arias Rivera, Jessica Esquivel Chahin, Shimon Shlomo Glick Betech and Sabrina Carriles Boro. (2023). Case Report: Resection of Giant Mediastinal Liposarcoma Using the Partial Sternotomy Incision, J. Clinical Case Reports and Studies 4(1); DOI: 10.31579/2690-8808/155
Copyright: © 2023 Jose Manuel Mier Ordionzola, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 November 2022 | Accepted: 13 December 2022 | Published: 28 January 2023
Keywords: liposarcoma; giant liposarcoma; mediastinal tumor; thoracic surgery
Primary mediastinal liposarcomas are rare. There are four types of liposarcoma: well differentiated/atypical lipomatous tumor, dedifferentiated, myxoid, pleomorphic. In this study we report a rare case of a mediastinal well-differentiated liposarcoma that was successfully surgically removed. Because of the noninvasive growth pattern of most liposarcomas, patients often present with few symptoms, which was the case in our patient presenting only with dry cough. Normally these tumors are diagnosed by radiologic imaging. Common symptoms include cough, dyspnea, wheezing, chest pain, and weight loss. There are different histologic variants of liposarcoma, the most frequent one is well-differentiated liposarcoma. In our case we couldn’t confirm the histology with fine needle aspiration but with the frozen section we confirmed the diagnosis of well-differentiated liposarcoma.
An optimal approach is very important to remove mediastinal liposarcoma because of the diversity of size and location of lesions.
Liposarcoma is one of the most prevalent malignant tumors developed from soft tissue, however, mediastinal liposarcomas as a primary tumor are very infrequent. Its most common location is the lower extremities and retroperitoneum [1]. When the primary liposarcoma is located at the mediastinum, it tends to grow insidiously from an expansive way instead infiltrative. Usually, these tumors leave no symptoms until its already taking pleural spaces or even compressing adjacent structures (such as Vena Cava) and the most common symptomatology is chest discomfort, dyspnea, and cough. Chemotherapy is ineffective for most cases of liposarcoma, that’s why the recommended approach is the surgical one, by a median sternotomy or lateral thoracotomy for the resection of the tumor. Is important to consider that large masses usually are complicated to manage by these approaches [2,3]. There is hardly any information and evidence about mediastinal liposarcomas since they are rare. According to the World Health Organization (WHO), there are four types of liposarcoma:
In this study we report a rare case of a mediastinal well-differentiated liposarcoma that was successfully surgically removed.
A 45-year-old woman, with no comorbidities presented to the external consultation with a dry cough of one year of evolution. The diagnostic approach was initiated with a computed chest tomography (CT) which revealed a large well defined mass. The mass extended from the anterior mediastinum in close relationship to the right common carotid artery and the right subclavian artery. The CT reported the mass of 17 x 11 cm in measurements (Figure 1). A CT-guided needle biopsy gave a report of undetermined histology. We preoperatively diagnosed liposarcoma or teratoma based on radiologic evaluation.
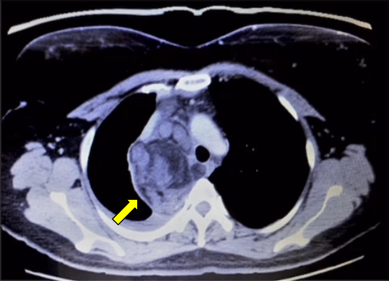
Figure 1: Presence of mass 17 x 11 cm in measurements localized in the mediastinum (arrow in yellow)
The operative management was first approached with a cervicotomy doing a frozen section of the mediastinal mass (Figure 2). The diagnosis was a liposarcoma in the frozen section. We continued the operative approach with a partial sternotomy incision (Figure 3).
Although the mass was wrapped around blood vessels, it did not invade adjacent structures including large blood vessels and could be removed en bloc.

Figure 2: Cervicotomy incision with a frozen section biopsy of the tumor.
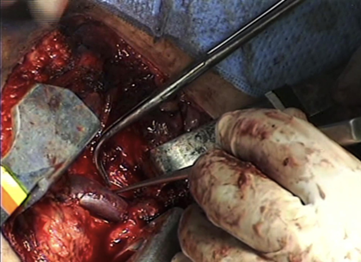
Figure 3: Partial sternotomy incision with dissection of vascular structures
The operation time was 5 h 30 min. Blood loss was 780 ml, including pleural effusion.
The resected specimen was an elastic hard, multilobular, and encapsulated yellow and gray mass. The tumor weighed 800 g with dimensions of 6 × 11 × 17 cm. The final histopathology confirmed well-differentiated liposarcoma. The patient tolerated the procedure well and had a postoperative recovery uneventful. Follow-up at 38 months showed the patient had a recurrence to the right lung which was treated with adjuvant radiotherapy, posteriorly the patient was disease free.
Liposarcoma is the most common soft-tissue sarcoma and accounts for approximately 20% of all mesenchymal malignancies [5]. About 90–95% of these tumors occur in the trunk, the extremities or retroperitoneum. Primary intrathoracic liposarcomas are unusual, representing 2.7% of all locations [6]. Some cases have been reported arising from the neck and subsequently spreading into the thoracic inlet, into the anterior or posterior mediastinum, matching the presentation in our patient [6].
Because of the noninvasive growth pattern of most of these tumors, patients often present with few symptoms, which was the case in our patient presenting only with dry cough. Normally these tumors are diagnosed by radiologic imaging. Common symptoms include cough, dyspnea, wheezing, chest pain, and weight loss [7].
There are different histologic variants of liposarcoma, the most frequent one is well-differentiated liposarcoma [1]. In our case we could not confirm the histology with fine needle aspiration but with the frozen section we confirmed the diagnosis of well-differentiated liposarcoma. The recommended therapeutic approach is surgical management. This is because liposarcomas have very low sensitivity to chemotherapy and radiotherapy [8].
For our case the partial sternotomy incision was chosen, this was because the tumor was localized in the right hemothorax with a cervical component. This allowed excellent visualization and complete dissection of the tumor. Partial sternotomy provides excellent exposure of both vascular and nonvascular structures allowing a safe access to the anterior superior mediastinum [9].
Long-term survival has been described to be dependent on encapsulated tumors and complete excision. Local recurrence is primarily related to the incomplete removal at the time of primary surgery [10].
In conclusion, an optimal approach is very important to remove mediastinal liposarcoma because of the diversity of size and location of lesions. The partial sternotomy incision provides a safe approach to the anterior mediastinum with an adequate visualization of the vascular structures. This approach can be used in selective patients and is an alternative for hemiclamshell or full sternotomy providing a less invasive approach.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
