
Case Report | DOI: https://doi.org/10.31579/2578-8965/174
Department of Obstetrics and Gynecology, Santokba Durlabhji Memorial Hospital and Research Center, Jaipur, India.
*Corresponding Author: Department of Obstetrics and Gynecology, Santokba Durlabhji Memorial Hospital and Research Center, Jaipur, India.
Citation: Brinderjeet Kaur, Anshu Sobhani (2023), Case Report on Misplaced and Malpositioned Fragmented IUCD, J. Obstetrics Gynecology and Reproductive Sciences, 7(4) DOI:10.31579/2578-8965/174
Copyright: © 2023, Brinderjeet Kaur. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 09 June 2023 | Accepted: 19 June 2023 | Published: 29 June 2023
Keywords: IUCD; fragmented IUCD; malpositioned IUCD; misplaced IUCD; uterine perforation
IUCD is one of the preferred forms of contraception that is reliable and cost effective. Nonetheless, IUCDs are not risk free and several complications have been reported, including unintended expulsion, misplacement and uterine perforation. Uterine perforation with an IUCD is uncommon, but it may have serious consequences including intra-abdominal bleeding, bowel or bladder perforation, fistula formation, especially when IUCD migrates to pelvic peritoneal spaces invading the adjacent organs.
It is rare for IUCD to break during removal and fragments lodged in uterine cavity. We present a case of retained fragment of IUCD which was diagnosed after 3 years of its so called ‘removal’. The case report emphasizes the need to train doctors not only to insert IUCD but also to educate the women about potential risks and benefits and self-examination of IUCD thread for its correct placement.
In developing country like India, IUCD are one among the most commonly used contraceptive methods from the cafeteria of available products. In fact, the use of long-acting contraception (LARC) especially intrauterine devices has dramatically increased over past few decades. IUCD are second preferred form of contraception and one of the most reliable and cheapest contraception methods. (1). IUCD has non contraceptive uses where it is used as treatment modality in conditions like abnormal uterine bleeding, heavy menstrual bleeding, Ashermanns syndrome and dysmenorrhoea. (2, 3) Nonetheless , IUCDs are not risk free and several complications have been reported , including unintended expulsion , misplacement , and uterine perforation (4) .The vast majority of misplaced IUCD s are found inside the uterine cavity or cervix rarely it may also perforate the uterine cavity or cervix .(5) Uterine perforation with an IUCD is uncommon , but it may have serious consequences including intraabdominal bleeding , bowel or bladder perforation , fistula formation , especially when IUCD migrates to pelvic peritoneal spaces invading the adjacent organs (5) . Rarely, at the time of IUCD removal, the device could break and the fragments of the IUCD could be left inside the uterine cavity.
We report a case of fragmented IUCD retained for six years after first removal which was retrieved by combination of hysteroscopy and use of IUCD hook.
A 33-year-old female presented with complaints of abdominal pain & fevers and was admitted in gasteroenterology department of our hospital. An immediate contrast enhanced computed tomography (CECT) was done revealed a cystic lesion in the lesser sac likely Lymphangioma and an incidental finding of IUCD in the lower uterine segment. A cross reference was sent to gynecology department for opinion and further management for IUCD. The in detail medical history revealed that she was having increased vaginal bleeding along with intermenstrual spotting for last 2 years.
The obstetric history of the patient brought to light history of two abortions followed by a normal full-term delivery of a female child five years ago. The patient underwent IUCD insertion immediately after delivery in post-partum period. Recently the patient got IUCD (Cu T) removed at a private hospital in a town near her village. As explained by the patient the removal was difficult causing her much pain however post operatively, she was shown the removed IUCD. This convinced her that IUCD has been removed successfully and she was trying to conceive for last 3 years but did not meet success. Her last menstrual period was 10 days back and had spotting off and on after that. She got her Cu T removal done at private hospital near her village, 3 years after the insertion. Thereafter her periods were normal for a year but later after a year had increased flow lasting for 4 days with intermenstrual spotting off and on and occurring every 28 days. She had full term vaginal delivery 8 years back and her daughter was healthy. Except of her present complaints of a pain abdomen and fever she gave no prior medical or surgical history.
CECT reports indicated a fragmented piece of IUCD in the lower segment of uterus.
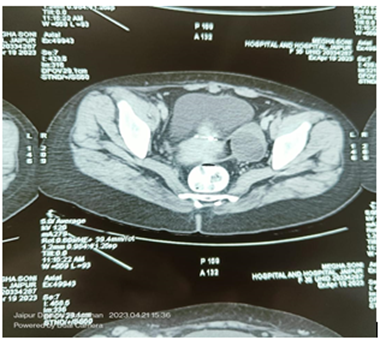
Figure 1: CECT showing fragmented piece of IUCD in the lower segment of uterus
(Figure -1) The patient and her husband were taken by surprise when we revealed that a portion of IUCD was still present in the uterus. On assimilating the news, and seeing her radiographic report, she came up with queries. Her concern for not being able to conceive and intermenstrual spotting. Both her concerns could be explained by the retained fragment of IUCD in the uterus. After taking informed consent and pre operative investigations as well as clearance from Gastroenterogist, the patient was posted for Hysteroscopic removal of IUCD.
She was given General anesthesia and was put in lithotomy position. Parts of the operative site, the perineal area and vagina were cleaned and painted with betadine and draped. Under aseptic precautions, bladder was emptied. Per vaginal examination was done. Uterus was normal and anteverted. Parts of Hysteroscope were assembled, Vaginoscopy was done followed by hysteroscopy to visualize the cavity of the uterus. The uterine cavity was normal in size and shape, bilateral ostia were normally located. However, no fragmented portion could be traced. While withdrawing the hysteroscopy, a hard structure was felt on the anterior aspect of the lower uterine segment (Figure-2, 3).
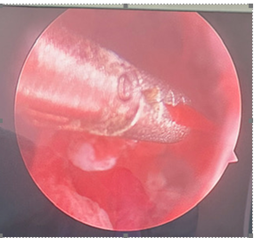
Figure 2: Hysteroscopy visualizing the embedded fragment of IUCD.

Figure 3: Hysteroscopy visualizing the embedded fragment of IUCD
As the IUCD was embedded in the myometrium an attempt was made with grasper to bring it into the uterine cavity. Repeated attempts were not enough. Then hysteroscope was withdraw and IUCD hook was used to move the hard part felt and the fragmented bit of IUCD successfully removed (Figure-4).

Figure 4: Hysteroscopy followed by IUCD hook assisted IUCD removal

Figure 5: The fragment of IUCD removed
Long active reversible contraceptives (LARC) are continually being used and are an effective option for preventing pregnancy. (6) Complications from retained IUCDs may be asymptomatic or symptomatic including cramping, ectopic pregnancy, embedment or fragmentation, expulsion, infertility, pelvic infection, uterine perforation and vaginal bleeding (7). Of late, fracture of the IUCD is a very rare complication (8) with a prevalence rate of 1-2 % . (9). Misplaced IUCD is termed as the condition when IUCD thread is not visualized through the cervical os . (10) Malpositioned IUCD is a condition where, although the IUCD is present within the uterine cavity but its placement is eccentric and part (fragmented) or the whole of it may be embedded in the myometrium. (11) Retained and fragmented IUCD is a very rare but a dangerous complication.
Research shows that an IUCD can be misplaced during years of use in the uterus due to anatomic, provider, or physiologic changes (12) Although research does not yet connect IUCD malposition to increased fracture risk this concern remains. With an IUCD moving beyond the original position, excess force and difficulty may occur in removing the device later, leading to potential fracture. Strong resistance encountered in removing IUCD may indicate the IUCD is embedded in the uterine wall. (13)
Malpositions of IUCDs were analysed by Zakin et al (14). According to them, the IUCD which penetrates only into the myometrium of the uterus are termed partial perforation. Such a position as shown in the fig -2 is position type - B. Following a Type –B perforation the IUCD lies entirely within the myometrium so that it cannot be seen either by hysteroscope or laparoscope.
Classification of partially perforated devices:
Type A: IUD present in the uterine cavity and myometrium
Type B: IUD present entirely in myometrium
Type C: IUD present in myometrium and peritoneal cavity
Type D: IUD present in all 3 compartments
Illustrative diagram of classification of partially perforated devices as proposed by zakin et al shown in figure-5.
The possible risk factors for uterine perforation have been proposed as – Insertion by less experienced clinician, lactation period, Postpartum insertion [< 6>
The patient did not suspect that she had retained fragment of IUCD, however on ultrasound would have been a good modality to identify the IUCD. Apart from the diagnosis of misplaced fragment of IUCD, CT scan imaging can precisely locate the migrating IUCD and help in planning and anticipating difficult removal. [16] Therefore in our case too we got CT scan done.
Current practice of removing IUCD is an office procedure. The IUCD is removed by securely grasping the strings at the external OS and applying traction [7] If resistance is met, then the removal should stop until the practitioner reassesses. [ 7] If the IUCD is not removed by conventional methods, dilatation of the cervix or ultrasound guidance should be considered. [7] Hysteroscopy should be reserved for removal of the retained IUCD after these methods have been tried. With lack of post operative complications after IUCD removal by hysteroscopy this method [11], as well as ultrasound guidance, might be a successful and cost effective first step in removal of IUCD in- patient or out -patient. In our case too, hysteroscopy was done to precise locate the embedded IUCD. This immensely helped in the retrieval of fragment of IUCD. Also, routine screening with ultrasound may need to be emphasized during routine care of patients. Facing too much resistance upon attempted removal of IUCD may warrant use of ultrasound or hysteroscopy. Further research considering improved stepwise removal should be considered.
In India, family planning is the need of the hour. It is therefore essential, that every effort should be made to bring down the failure and complication rates of the contraceptive measures, so that more couples are encouraged to use this method for contraception. IUCD being safe, cost effective, user-friendly, one-time application, hassle free method, caregivers should ensure that a mere insertion is not the end point of their services. Educating the women of the potential benefits, the complications of the device, IUCD care and regular follow up should be mandatory. Proper training of the health professionals in terms of patient selection, technique of insertion, identification of danger signs, diagnosing and management of complications of IUCD should be made mandatory, so that they are able to provide better family planning services.
Nil
Nil
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
