
Case Report | DOI: https://doi.org/10.31579/2690-4861/292
Head of Cardiology department, Alshifa Hospital, Gaza, Palestine, A.Professor, Faculty of Medicine, IU Gaza , Palsetine.
*Corresponding Author: Head of Cardiology department, Alshifa Hospital, Gaza, Palestine, A.Professor, Faculty of Medicine, IU Gaza , Palsetine.
Citation: Mohammed Habib, (2023), Case Report of New Technique for the Repair of Iatrogenic Femoral Pseudoaneurysm. International Journal of Clinical Case Reports and Reviews. 13(2); DOI: 10.31579/2690-4861/292
Copyright: © 2023 Mohammed Habib, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 January 2023 | Accepted: 01 February 2023 | Published: 15 February 2023
Keywords: femoral artery pseudoaneurysm; star close
Femoral artery Pseudoaneurysm was caused at the puncture site of the right groin after diagnostic coronary angiography. Manual compression for 48 hours was administrated but failed then balloon tamponade was attempted for hemostasis at the aneurysmal site but hemostasis was not achieved. Next, using contralateral anterograde approach was use to cross the wire from the neck of the pseudoaneurysm and ipsilateral retrograde approach by direct puncture of the pseudoaneurysm was tried. A 0.014-inch guidewire was crossed from the neck of the pseudoaneurysm to the external iliac artery. The wire was replaced with a 0.035-inch guidewire. A star close device was inserted and was deployed at the neck of the pseudoaneurysm. Final angiography revealed completion of hemostasis.
Femoral artery access is the most common approach for diagnostic and therapeutic coronary intervention. However, puncture site complications, such as Fistula, bleeding, hematoma and pseudoaneurysm may occur [1]. Pseudoaneurysm is the most common femoral access complication following coronary and peripheral angiography and/or angioplasty, incidence ranges from 0.2percentage to 8percentage [2]. Risk factors include antiplatelet agents, anticoagulants, larger sheath size, puncture site below common femoral artery, and emergency procedures.
Symptoms may include groin swelling, unusual pain, bruising, skin changes, neuropathy from femoral nerve compression, and, rarely, limb ischemia or claudication from embolization or arterial compression. Rupture can be associated with severe pain and hemodynamic instability. Hence, interventional cardiologists should be familiar with management. The most common nonsurgical treatment options are duplex ultrasound-guided compression, duplex ultrasound-guided Sealing pseudoaneurysms of the femoral artery with saline injection and duplex ultrasound-guided thrombin injection, which are widely used and fairly successful [3]. However, a novel approach with suture-based closure devices to treat pseudoaneurysms was recently reported [4]. In this case report, we describe the off-label use and the long-term outcome of the Angio-Seal vascular closure device to repair a femoral pseudoaneurysm. We use new technique by using star close device with contralateral and ipsilateral approach to close the neck of the femoral pseudoaneurysm. obtained informed consent of the patient for publication of this case report.
A 42-year-old male who underwent angiography with no obstructive disease found. he was discharged home on the same day but returned to the hospital for Symptoms include groin swelling, unusual pain, bruising, skin changes, neuropathy from femoral nerve compression and claudication from embolization or arterial compression. On examination pulsatile mass in his right groin with a bruit. Angio CT suggested large pseudoaneurysm 7x8 cm in right femoral artery (figure1). Angiography to his right common femoral artery revealed large pseudoaneurysm [2]. With a contralateral sheath placed in the left common femoral artery, the pseudoaneurysm was entered through the neck using 0.014-inch coronary wire. A micro introducer needle was then used to enter the pseudoaneurysm A 0.014-inch wire was then advanced through the neck of the pseudoaneurysm retrogradely into the external iliac artery. The micro introducer sheath was then advanced into the pseudoaneurysm over the wire and retrogradely into the external iliac artery. The 0.014-inch wire was exchanged with a 0.035-inch Whole wire. The star closure device was then deployed with the anchor against the pseudoaneurysm neck with subsequent thrombosis of the pseudoaneurysm (figure 3). Control Angiography through the contralateral sheath showed complete occlusion of the neck with no compromise to the common femoral artery.
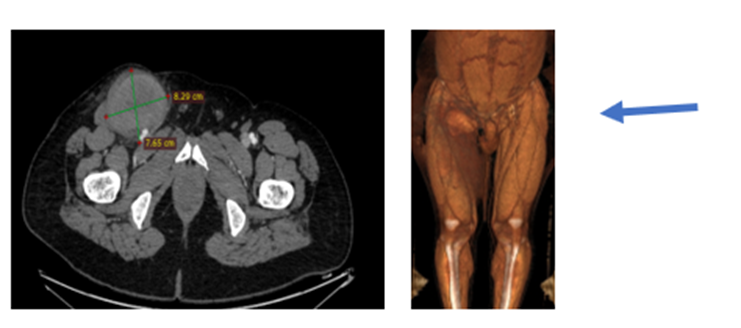
Figure 1: CT angiography: large pseudoaneurysm in right femoral artery
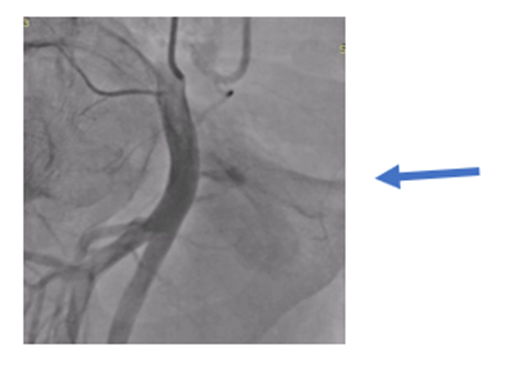
Figure 2: Selective angiography: pseudoaneurysm in right femoral artery

Figure 3: after star close deployment, totally occlusion in pseudoaneurysm neck
In this case, a novel approach to close an iatrogenic pseudoaneurysm using the star closure device. This alternative method is likely to be useful in the setting of a large pseudoaneurysm (> 3 mm) with a neck diameter less than 5 mm.
The Alshifa Hospital new technique of treatment for femoral artery pseudoaneurysm involved 4 steps to closure the neck of femoral artery pseudoaneurysm.
1.contralteral anterograde via 3.5,6 French right Judkins guiding catheter 0.014-inch wire insertion into the femoral artery pseudoaneurysm. (Figure 4)
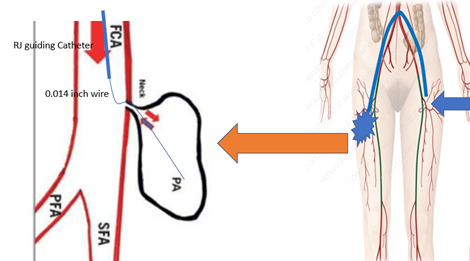
Figure 4: SFA: superficial femoral artery, PFA: deep femoral artery, FCA: Common femoral artery, PA: Pseudoaneurysm
2. ipsilateral retrograde via direct puncture 0.014-inch wire insertion into the external iliac artery through neck of pseudoaneurysm (figure 5)
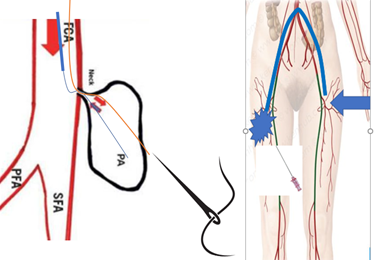
Figure 5: SFA: superficial femoral artery, PFA: deep femoral artery, FCA: Common femoral artery, PA: Pseudoaneurysm
3.The 0.014-inch wire was exchanged with a 0.035-inch Whole wire. The introducer sheath was then advanced into the pseudoaneurysm over the wire and retrogradely into the external iliac artery (figure6)
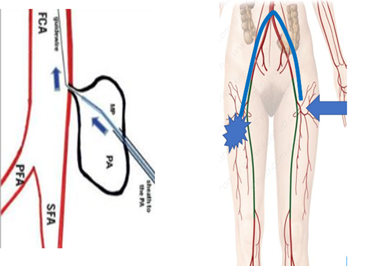
Figure 6: SFA: superficial femoral artery, PFA: deep femoral artery, FCA: Common femoral artery, PA: Pseudoaneurysm
4.The (star close device/or Angio cell device) was then deployed with the anchor against the pseudoaneurysm neck with subsequent thrombosis of the pseudoaneurysm (figure 7)
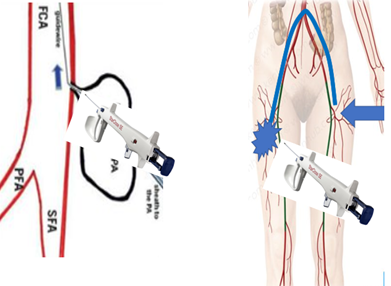
Figure 7: SFA: superficial femoral artery, PFA: deep femoral artery, FCA: Common femoral artery, PA: Pseudoaneurysm
Femoral artery pseudoaneurysm is the most common complication of coronary and peripheral intervention. the incidence of pseudoaneurysm at 0.2percentage to 0.5percentage following diagnostic procedures and up to 8percentage following procedures with an intervention [2]. Conservative management is an option for some patients with small femoral artery pseudoaneurysms.
ultrasound-guided compression was used to treat pseudoaneurysms, replacing surgical procedures for many pseudoaneurysms and reporting an early success rate of 63percentage to 88percentage [4]. Ultrasound-guided thrombin injection has replaced ultrasound-guided compression in most practices. Injection has a success rate of 93percentage to 97percentage, compared with 63percentage to 88percentage for ultrasound-guided compression. Complications of ultrasound-guided thrombin injection are rare (1.2percentage), with the most common being distal embolization (0.5percentage) [5].
Patients with large hematomas resulting in compressive symptoms such as neuropathy or ischemia and infected pseudoaneurysms are best treated with surgical repair. Surgical treatment carries a significant complication rate of 20percentage [6].
Our new technique has several advantages. high success rate and the most patients who are currently undergoing treatment with oral anticoagulants and antiplatelet agents can be successfully treated because the vascular closure device is effective independent of concomitant medications. However, we believe that this technique may be superior to thrombin
injection because potential complications that might occur with thrombin injection, such as peripheral embolism of thrombin or anaphylactic reactions, are avoided, and it is less invasive than open repair.
This article's completion was not supported by any money.
The author has no financial or non-financial interests to report.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
