
Case Report | DOI: https://doi.org/10.31579/2690-1897/149
Royal Darwin Hospital in Northern Territory Australia.
*Corresponding Author: Misha Lay, Royal Darwin Hospital in Northern Territory Australia.
Citation: Misha Lay, Philip Toonson., (2023), Case Report of Chylous Ascites as A Complication of Severe Necrotising Pancreatitis, J, Surgical Case Reports and Images 6(3); DOI:10.31579/2690-1897/149
Copyright: © 2023, Misha Lay. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 February 2023 | Accepted: 14 March 2023 | Published: 22 March 2023
Keywords: chylous ascites; chyle; acute pancreatitis; pseudocysts; necrotising pancreatitis; gallstones pancreatitis
Chylous ascites (CA) in the setting of acute necrotising pancreatitis is a rare clinical entity, with its pathogenesis and optimal management remaining uncertain. In Western countries, CA is most commonly attributed to malignancy, liver cirrhosis and trauma causing direct disruption to the lymphatic system leading to the leakage of chyle into the peritoneum. This case report describes a middle-aged woman who develops chylous ascites a few months after an episode of severe acute necrotising pancreatitis secondary to gallstones, complicated by infected pancreatic pseudocysts. She underwent a paracentesis, octreotide and strict dietary modifications of a low-fat and high-protein diet with effective clinical resolution of her chylous ascites. Although multiple management options for chylous ascites exist and have been explored in the limited available literature, the emphasis remains to be placed on identifying and treating its underlying aetiology.
Chylous ascites(CA) in the setting of acute necrotising pancreatitis is a rare clinicalentity [1]. The phenomenon is characterised by the accumulation of ascitic fluid containing chyle,a lipid- rich lymph fluid within the peritoneal cavity, resulting in abdominal distension and often discomfort for the patient [2]. CA is a manifestation of an underlying aetiology that causesan obstructive or traumatic disruption to the lymphatic system that ultimately leads to the leakageof chyle [2], and often portends nutritional, immunological and mechanical consequences [3]. In Western countries, it is primarily attributed to malignancies such as lymphoma, liver cirrhosis, and blunt or surgical trauma to the abdomen or retroperitoneum [3]. Congenital lymphatic anomalies in children and Mycobacterium and filariasis infections in developing countries have also been widely recognised, converse to acute pancreatitis which has rarely been recognised in published literature [2]. The pathogenesis of CA in acute pancreatitis is poorly understood, and its optimal management remains uncertain [3]. This case report describes a middle-aged woman who develops CA after a prolonged hospital admission for severe necrotising pancreatitis secondary to gallstones,and it explores her course of management and outcome. Preceding the development of CA, the patient’s clinical course was complicated by the development of infected pancreatic pseudocysts requiring percutaneous drainage and long-termantibiotics. The patientultimately required re- admission to hospital for her CA, which was managed with a therapeutic paracentesis, low- fat and high-protein modified diet, and octreotide with effective clinical improvement.
A middle-aged woman presents to the ED with jaundice, epigastric pain radiating to her back,diarrhoea,vomiting,and subjective fevers.She has a background of hypertension that is well-managed with irbesartan.The patient is a non-drinker and non-smoker,and there is no prior history of cholelithiasis. On review,she is jaundiced,tachycardic with a HR of 100bpm,normotensive BP 120/70,tachypnoeic RR 28bpm,SpO2 93% on FiO2 0.21,apyrexicand anuric with only 10mL of dark urine passed in prior 12 hours.There was tenderness on palpation of the epigastrium which radiated to her back and left shoulder on examination.Her blood investigations demonstrated raised inflammatory markers of WCC 27.6 and CRP 273.7.She had a raised lipaseof 9473 with an associated liver derangement with Br 230 ALP 98 GGT 286 ALT 370. There was a concurrent metabolic acidosis,anuric renal failurewith a raised creatinine of 653 and uraemia of 30.1. A non-contrast CT abdomen and pelvis (see Figure 1) was performed and demonstrated diffuse enlargement of the pancreas, particularly in the head and neck with marked peripancreatic fat stranding.
Appendix
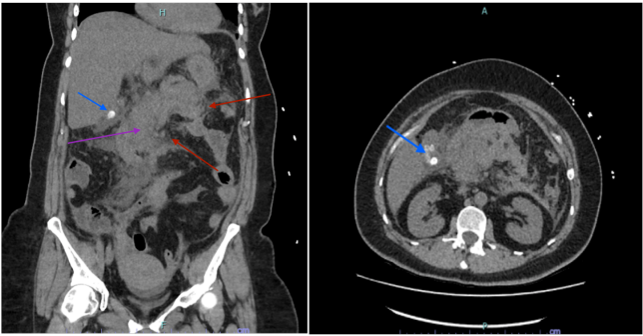
Figure 1: CT abdomen and pelvis coronal view (left) demonstrating generalised oedema of the pancreas (purple arrow) with peripancreatic stranding (red arrows). In the coronal and axial view (right), multiple gallstones can also be seen within the gallbladder (blue arrow) without evidence of cholecystitis.
There is also free fluid tracking into the paracolicgutters, and small amounts of scattered intraperitoneal fluid. Multiple gallstones are present in the gallbladder without any signs of cholecystitis or a dilated CBD.The patient was diagnosed with severe acute necrotising pancreatitis presumed secondary to gallstones,with an associated acute anuric kidney failure and ModifiedGlasgow Score of 3.
The patient was admitted to ICU for management of her anuric acute renal failure with CRRT. Her ICU stay was further complicated by fluid overload, bibasal pleural effusions and atelectasis requiring invasive ventilatory support for respiratory failure for a few days. She progressively improved with supportive measures over the course of a week and was discharged from the ICU to the ward. She further developed persistent pyrexia on the ward with raising inflammatory markers prompting a repeat CT abdomen and pelvis which identified multiple peripancreatic collections presumed to be evolving pseudocysts. An IR- guided percutaneous drainage of the pseudocysts with a 14Fr pigtail drain insertion was subsequently performed (see Figure 2) with frank haemopurulence output that grew E. coli and candida species.

Figure 2: CT abdomen and pelvis coronal (left) and axial (right) views demonstrating multiple infected post-necrotic peripancreatic fluid collections (red arrows) approximately 2 weeks after admission for severe necrotising pancreatitis.
Clinical improvement was achieved afterwards with IV antibiotics administration and the patient was deemed fit for dischargewith the pigtail drain kept in situ with plans for out patient clinic reviews and serial imaging. On outpatient clinic reviews, the patient had persistently high drain outputsand was commencedon regular creonwith meals whilst awaiting further discussions about the benefits of a video-assisted retroperitoneal debridement to be performed at an interstate hospital.
Approximately 3 months since discharge from hospital, the patient presents to the outpatient clinic with a new abdominal distension and discomfort that was not present during her prior clinic review 3 weeks ago. On examination, she had large ascites with minimal tenderness and no signs of peritonism. Her existing pigtail drain output for the peripancreatic pseudocysts was otherwise weaning in volume. The patient was re-admitted to hospital for further evaluation where she underwent another CT abdomen and pelvis scan which demonstrated new large-volume ascites (see Figure 3)
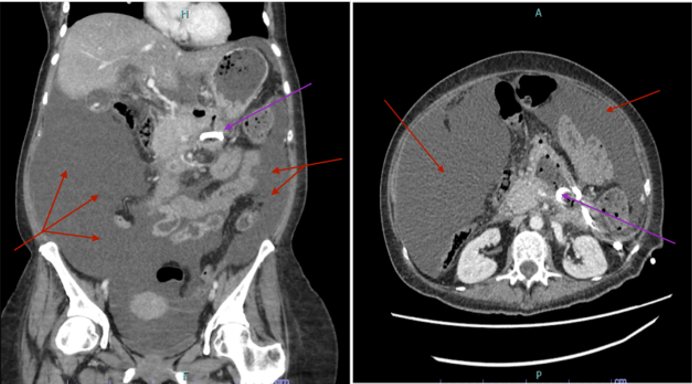
Figure 3: CT abdomen and pelvis coronal (left) and axial (right) views demonstrating large volume ascites (red arrows). The pigtail drain (purple arrow) situated in the peripancreatic space is left in situ with residual pseudocysts present.
The patient had no evidence of liver cirrhosis to explain the ascites. An IR USS-guided ascitic tap and 8.5Fr drain insertion was performed, with milky opaque fluid drained and sent for analysis. The fluid analysis demonstrated high triglycerides of 10.03 mmol/L and low cholesterol of <1>The management of the patient’s CA was primarilywithin the outpatient setting, with ongoingdietician input to ensure adequate nutritional demands are met and maintained from the ongoing chyle leak.
The patient improved clinically on a low-fat and high-protein diet, with resolution of her hypoalbuminaemia, resultant weight gain and improvement of her CA as demonstrated by her reducingdrain output and serial CT scan (see Figure 4).

Figure 4: CT abdomen and pelvis coronal view after therapeutic percutaneous drainage andinsertion of pigtail drain located in the lower left quadrant (light blue arrow). It demonstrates reduced volume of ascites (red arrow).
The drain output weaned down to 50mL/24 hours at approximately 1 month from the drain insertion. The drain inadvertently blocked and was removed without a re-accumulation of the chylous ascites. The peripancreatic pseudocysts also simultaneously receded on serial CT scans and the drain was removed. The patient reconditioned, gained some weight and was slowly re-introduced to higher fat-content foods such as lean meats, butter and mayonnaise prior to an eventual upgrade to a normal diet with no re-accumulation of her ascites. She also fortunately had no evidence of exocrine or endocrine pancreatic insufficiency following her severe episode of pancreatitis. The patient ultimately underwent an elective laparoscopic cholecystectomy which identified small residual volumes of chylous ascitic fluid (see Figure 5).
Figure 5: Photograph of residual chylous ascitic fluid identified during elective laparoscopic cholecystectomy, demonstrating its milky and opaque characteristic appearance.
CA in the context of acute pancreatitis and its optimal management is poorly understood [7]. It is defined as the presence of milky fluid with high triglycerides of over 110mg/dL within the peritoneal cavity [8]. There are multiple proposed approaches to classifying the aetiologies for CA, such as by traumatic or atraumatic groups [2], or by the presence or absence of associated portal hypertension [5]. The pathogeneses can furthermore be categorised into main mechanisms that include obstruction to lymph flow such as from an extrinsic compression from a tumour, exudation of lymph through walls of dilated retroperitoneal vessels, traumatic disruption to the thoracic duct and leakage through a lymphoperitoneal fistula [8]. However, the pathogenesis of chylous ascites in acute pancreatitis remains uncertain due to the limited literature available recognising it as an aetiology of CA [3].
It is speculated in this case whether the development of chylous ascites in the context of necrotising pancreatitis is attributed to the leakage of pancreatic autodigestive enzymes leading to direct erosion into the surrounding pancreatic and peripancreatic lymphatic channels, similarly to the pathogenesis of haemorrhage in pancreatitis with disruption to surrounding blood vessels. It is recognised that the abundant lymphatic chains surrounding the pancreas increase in lymph flow during episodes of pancreatitis [9]. However, the patient developed chylous ascites months from her episode of severe acute necrotising pancreatitis and development of pseudocysts, challenging this mechanism.
The optimal management of chylous ascites unsurprisingly remains unclear, with existing case studies identifying various regimens and clinical outcomes that appeared individualised. The mainstay management is paracentesis, dietary modifications, somatostatin analogues, and consideration of total parental nutrition and diuretics [4]. It is emphasised that clinicians should identify and treat the underlying aetiology [6] and recognise that atraumatic aetiologies should warrant exclusion of other aetiologies such as malignancy [1]. In this case, the patient had no evidence of cirrhosis or malignancy on formal investigations, with her recent acute necrotising pancreatitis being the most likely cause of her CA. She ultimately underwent an elective laparoscopic cholecystectomy to prevent further gallstone pancreatitis episodes as her chylous ascites was secondary to her necrotising pancreatitis and pseudocysts. Pharmacological agents such as somatostatin and its analogues, octreotide have been recognised to reduce intestinal, splanchnic and portal blood flow hence chyle excretion, and have been utilised in similar reported cases with clinical improvement [5].
For medically refractory patients, some case studies have described improvement from vigorous dietary modifications of fasting the patient and administering total parental nutrition for weeks duration [4]. In unique circumstances where patients remain refractory to vigorous conservative management, surgical interventions such as a transjugular intrahepatic portosystemic shunt (TIPS), peritoneovenous shunt, embolisation or exploratory laparotomy may be considered however is dictated by the aetiology of the CA [3]. The patient described in this case report avoided surgical intervention, as she demonstrated a favourable clinical response to a single paracentesis with pigtail drain insertion, low-fat and high-protein dietary modifications and octreotide. She also fortunately did not develop any pancreatic insufficiency or any permanent organ dysfunction after her episode of severe necrotising pancreatitis.
Chylous ascites (CA) is a rare manifestation of chyle accumulation within the peritoneum that has been rarely attributed to acute pancreatitis. The patient in this case report develops chylous ascites after an episode of severe necrotising pancreatitis secondary to gallstones, which was effectively managed with a therapeutic paracentesis, octreotide and strict dietary modifications with a low-fat and high-protein diet. It is emphasised that clinicians should focus to identify and treat the underlying aetiology of CA, and exclude sinister aetiologies such as malignancy especially in cases of atraumatic CA. Although the optimal management of CA remains poorly understood, the mainstay management is dietary modifications to reduce chyle leak and counteract resultant malnutrition and consider pharmacological therapies such as somatostatin analogues and diuretics. In unique circumstances where patients are refractory to conservative management, consideration of surgical interventions such as TIPS, embolisation and exploratory laparotomy may be undertaken.
CA – Chylous Ascites.
HR – Heart Rate.
BP – Blood pressure.
WCC – White cell count.
CRP – C-reactive protein
LFT – Liver Function Test.
ICU – Intensive Care Unit.
IR – Interventional Radiology.
USS – Ultrasound.
CRRT – Continuous Renal Replacement Therapy.
CT – Computedtomography.
TPN – Total Parental Nutrition.
TIPS – Transjugular Intrahepatic Portosystemic Shunt
No conflicts of interest identified.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
