
Case Report | DOI: https://doi.org/10.31579/2690-4861/335
Department of General Surgery and College of Health Sciences and Medicine, WOLAIAT Sodo University, Ethiopia.
*Corresponding Author: Louis Marko LEMI, and College of Health Sciences and Medicine, WOLAIAT Sodo University, Ethiopia.
Citation: Natinael Sima, Louis M. Lemi, Maku S. Bokasoro, (2023), Case Report: Incidental Littoral Cell Angioma of The Spleen [Benign Splenic Tumor], International Journal of Clinical Case Reports and Reviews, 14(4); DOI:10.31579/2690-4861/335
Copyright: © 2023, Louis Marko LEMI. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 August 2023 | Accepted: 08 September 2023 | Published: 15 September 2023
Keywords: splenectomy; laparotomy; littoral cell angioma; splenic tumor; abdominal mass
littoral cell angioma is an unusual benign tumor of the spleen and is primary splenic vascular tumor arises from the normal littoral cells lining the sinus channels of the splenic red pulp we are report a case of 17 years male boy have history of abdomen pain for 2day with fever and he was managed with laparotomy and splenectomy and Postoperative pathology biopsy examination confirmed the final diagnosis of LCA of spleen.
Spleen tumors are infrequent and are classified as lymphoid or nonlymphoid. Splenic lymphoid tumors are mostly Hodgkin disease or non-Hodgkin lymphoma. These tumors are uncommon as primary spleen lesions; nevertheless, the spleen is frequently the location of subsequent involvement. Lymphoid lesions appear first in the white pulp, whether primary or secondary. The process might be diffuse, as in nodular lymphoma, or limited, as in big irregular lymphomas. In the event of Hodgkin disease, surgical treatment always includes a complete splenectomy, either as part of a staging surgery or as an effort at cure [1].
A 17-Year-old Ethiopian male come to the emergency department with a history of abdominal pain for 2day started at left upper quadrant and become diffuse all over the abdominal and associated with high grade fever and chills and no history of vomiting and no bowel change habit and no history of weight loss and no history of abdominal trauma he has history of abdominal pain for last 6 week subside without treatment and no chronic conditions.
On examination look unwell, temperature is 38.4C, pulse 115/minute, blood pressure 125/75 mm Hg, respiratory rate 20/minute. There was no jaundice and no cyanosis a. and not pale the abdomen was diffuse tenderness over all abdominal with palpable mass at left subcostal region and have hypoactive bowel sound, A complete blood cell count was done is showing below in the tab.
| Tests ordered | Result | Reference value |
| WBC count | 9.7 | 4.200- 11,000/mm3 |
| Differential count | ||
| Neutrophil | 81.7 | 40-74% |
| lymphocytes | 11.7 | 21-40% |
| Monocytes | 1 | 2-10% |
| Eosinophil | 1.1 | 1-6% |
| basophile | 0.5 | 0-1% |
| RBC | 5.1 | 3.8-5.6 M/UL |
| Hemoglobin | 12 | 12-18 g/dl |
| hematocrit | 40.5 | 30-57% |
| MCV | 81 | 80-97FL |
| MCH | 24 | 26- 32Pg |
| MCHC | 29.6 | 31-36g/dl |
| Platelet | 186 | 150-450 OK/UI |
He was admitted for surgery with impression of generalized peritonitis 2rd to splenic abscess?? And intravenous normal saline 0.9% was started and intravenous ceftriaxone was given, informed consent was obtained and patient transfer to major operation room under general anesthesia. The abdomen was open through a midline incision, about 800ml of heamarrgic peritoneal fluid were drained and found huge splenic mass size is[ 25 x 30] arise from the lower pole of spleen no attachment with near structures [stomach and pancreas left kidney and left colon] and there is minimal mesenteric lymph node enlargement at proximal small bowel, and mobilization of spleen by transection of ligamentous attachments , superior pole include the splenophrenic ligament and the splenocolic and splenorenal ligaments at the inferior pole and the lateral attachment were dissected by blunt dissection , and the ligation of short gastric was done and splenic vessels was ligated separated at tail of pancreas and splenectomy was done and the drainage was left in situ and biopsy was sent all the rest of the organ were normal and small bowel and large bowel was repositioned and the abdomen was closed in layers. The patient tolerated the procedure well.
On the second postoperative the diet was initiated and the drainage output is about 150ml the incision site was clean and on five postoperative the drainage was removed, and postoperative CBC was normal.
On seventh postoperative day he was discharged and follow up after one months he was doing well and the biopsy results was report [microscopy–sections show irregular tortuous blood- filled vascular channels lined by plump endothelial cells form papillary projections into Lumina, sloughing of endothelial cells into vascular noted, no features of malignancy noted all four lymph nodes identified show reactive feature of sinus histiocytosis only, index littoral cell angioma of spleen.
The intraoperative finding is showing below figure [1, 2, 3, 4].

Figure 1: intraoperative finding showing huge splenic mass [Credit; Dr Temesgen Hitiso].

Figure 2: intraoperative showing the short gastric vessel dissection and ligation and tail of pancreas [Credit; Dr Asmare walle].
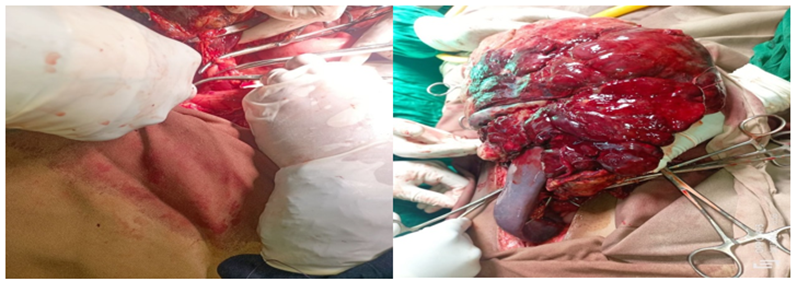
Figure 3, 4: intraoperative showing ligation of splenic vessels and splenectomy [Credit Dr; Eyosiyas shimels].
Falk et al. originally reported littoral cell angioma of the spleen as an uncommon vascular tumor. Littoral cells in the splenic red pulp sinuses give rise to the tumor. Littoral cell angioma affects both men and women equally and has no age preference. It is frequently asymptomatic and discovered by chance. Some patients with littoral cell angioma may exhibit hypersplenic symptoms such as anemia, thrombocytopenia, and splenomegaly, the latter of which is seen in nearly all patients with this condition [2]. discovered that 17% of LCA cases were associated with immunological or congenital disorders such as Crohn's disease, Wiskott-Aldrich syndrome, Epstein syndrome, lymphocytic colitis, ankylosing spondylitis, Gaucher's disease, myelodysplastic syndrome, chronic glomerulonephritis, or aplastic anemia. Only after surgery is it possible to make a definitive diagnosis [3], Because of the paucity of instances, the origin and natural history of LCA are unknown and [4] Although the majority of littoral cell angiomas documented in the literature have been proven to be benign, this tumor condition has no distinctive symptoms Pressure pain in the left subcostal region, mesogastrium, and splenomegaly are examples of symptoms that can be noticed during a clinical examination. The blood count may be fully normal, although anemia, thrombopenia, or even a pancytopenia image is frequently present with hypersplenism. Ultrasound is the first-line imaging technique, and it is best when combined with a contrast agent. If diagnostic doubt continues, computed tomography or magnetic resonance imaging with a contrast agent is the next step [2, 5] and two case reports have described LCA variants with malignancy-like histopathological characteristics [6, 7], Littoral cell angioma is an uncommon benign tumor that develops from the cells lining the red pulp and can cause splenomegaly Both benign conditions are treated symptomatically, with observation for small asymptomatic lesions and total splenectomy for larger symptomatic hemangiomas a, Percutaneous biopsy of splenic tumors is not recommended due to the risks of bleeding, tumor seeding, and uncertainty of diagnosis on fine- or core-needle specimens. A total splenectomy is the greatest way to obtain safe and effective surgical procedures for primary splenic tumors, as the majority of the littoral cell angiomas reported in, so far, just one case of partial splenectomy has been described [1, 8]. A retrospective study was conducted, which revealed that laparoscopy is an alternative for LCA management [9], A large number of LCA patients who undergone splenectomy were at risk of long-term consequences such as sepsis, thrombosis, and tumor [10].
LCA is an uncommon benign splenic tumor that can be diagnosed postoperatively via biopsy and treated with a total or partial splenectomy. As well as close postoperative monitor.
Nil.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
