
Case Report | DOI: https://doi.org/10.31579/2690-8808/156
1 Founder and Medical Director- Institute of Minimally Invasive Thoracic Surgery, Hospital Angeles Lomas, Mexico City, Mexico. Vialidad de la Barranca 240, Hacienda de las Palmas, Huixquilucan, Estado de México 52763. 5521078324.
2 Department of General Surgery, Hospital Angeles Lomas, Mexico City, Mexico.
3 Doctor of medicine and Medical Assistant- Institute of Minimally Invasive Thoracic Surgery, Hospital Angeles Lomas, Mexico City, Mexico.
*Corresponding Author: Jose Manuel Mier Ordionzola, Founder and Medical Director- Institute of Minimally Invasive Thoracic Surgery, Hospital Angeles Lomas, Mexico City, Mexico. Vialidad de la Barranca 240, Hacienda de las Palmas, Huixquilucan, Estado de México 52763. 5521078324
Citation: Jose Manuel Mier Ordionzola, Atl Simon Arias Rivera, Jessica Esquivel Chahin, Shimon Shlomo Glick Betech and Sabrina Carriles Boro. (2023). Case Report: Cardiac Metastases in a Non-seminomatous Tumor. J, Clinical Case Reports and Studies 4(3); DOI:10.31579/2690-8808/156
Copyright: © 2023 Jose Manuel Mier Ordionzola, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 November 2022 | Accepted: 13 December 2022 | Published: 16 February 2023
Keywords: non-seminomatous tumor; metastases; mediastinal tumor; cardiac effusion
Germ cell tumors are the most prevalent malignancy in young males commonly formed in the testicles. Primary mediastinal non-seminomatous germ cell tumors are rare, they tend to be aggressive and have unsatisfactory outcomes. Non-seminomatous cell tumors, it is the most likely testicular cancer to cause metastasis. Symptoms such as giddiness, fainting, fatigue, shortness of breath and chest discomfort are potential presentations in the emergency department on cardiac metastases. Primary mediastinal non-seminomatous germ cell tumor are considered high risk. Treatment is based on the underlying pathology, usually chemotherapy followed by surgery. Rare cases like this need to be reported and further studied to give patients better expectancy when diagnosed. The bad surveillance rate of 40 to 45% survival at 5 years and less than 10% overall is mostly due to the lack of response to aggressive chemotherapy and the concomitant pathologies that this presentation.
Germ cell tumors are the most prevalent malignancy in young males commonly formed in the testicles [1]. Some risk factors associated to testicular cancer include, cryptorchidism, hypospadias, decreased spermatogenesis evidenced by subfertility or infertility, familial history of testicular tumors in first-degree relatives, childhood inguinal hernias, pediatric atrophic testis and germ cell neoplasia in situ (GCNIS) [2]. Germ cell tumors can be found outside the gonads, either in the mediastinum (approximately 2-4% of all germ cell tumors), or in the retroperitoneum [1]. Mediastinal germ cell tumors are associated with Klinefelter Syndrome and hematologic cancer, there are three types according to their histology: seminomas, non-seminomatous tumors, and teratomas [3]. Primary mediastinal non-seminomatous germ cell tumors are rare, they tend to be aggressive and have unsatisfactory outcomes [4].
Patient with localized testicular cancer typically present with painless nodule, lump, mass, or swelling in one of the testes [2]. Non-seminomatous germ cell tumors (NSGCT) are associated with male infertility due to low sperm counts, reduced sperm motility, and increased abnormal morphology.[2] Systemic symptoms include anorexia, malaise, and weight loss [5].
Metastatic cardiac tumors are uncommon and infrequent, they can arise from any cancerous tumor, however, the evidence shows that mainly they derive from melanoma, leukemia, lymphoma, lung cancer carcinoma, renal cancer, and soft tissue sarcoma [6,7]. Some common symptoms of metastatic cardiac tumors are chest pain, dyspnea, cough, wight loss, superior vena cava syndrome, fever and nausea [5]. Testicular NSGCT most frequently metastasizes through the lymphatics to the retroperitoneum and may subsequently metastasize to contiguous mediastinal lymphatics, but it may also spread to brain, lungs and bone through different lymphatic pathways [8].
In this study, we report a case of cardiac metastasis originated from a primary mediastinal non-seminomatous germ cell tumor, there are very few studies which have reported clinical outcome and its treatment.
A Patient of 40 years of age with a previously known diagnosis of a non-seminomatous tumor, treated with chemoradiation and surgery. He arrived at the emergency department with chest pain of oppressive characteristics that initiated 4 days ago, which posteriorly was accompanied by tachycardia and dyspnea. At the physical exploration, the patient had tachycardia of 120 beats per minute, with the rest of the vital signs without alteration. The pulmonary exploration was positive for pleural effusion, we proceeded with the diagnosis approach with a thorax computed tomography. The study revealed bilateral pleural effusion with the presence of pericardial effusion and a conglomerate of tumoral mass in the mediastinum (Figure 1). We posteriorly did a transthoracic echogram that evidenced the presence of pericardial effusion of 500 ml and 3 masses in the pericardial space of 30 x 25 mm of dimensions (Figure 2). The patient was programmed for a left thoracoscopy. In the operation, we encountered multiple adherences between the chest wall and lung and changed the surgical approach to left thoracotomy. We posteriorly did a pericardial window and drainage of pericardial effusion. During the operation, there were multiple tumor metastases in the parietal pulmonary pleura, pericardial space, and cardiac tissue (Figure 3). A chest drainage was left in place and sent the tumor metastases to pathology. The final diagnosis of pathology was a metastasis of persistent mediastinal primary non-seminomatous germ cell tumor (Figure 4). In the post-surgical time, the patient had a torpid evolution, for which reason palliative therapy was decided. The patient posteriorly died because of his poor prognosis.
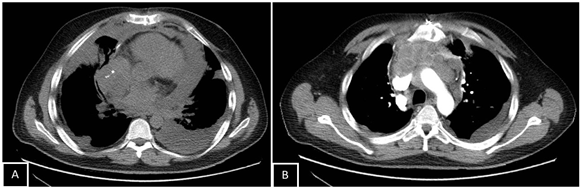
Figure 1: Inferior paratracheal and right lobar mediastinal adenopathies up to 17 mm were identified.

Figure 2: Presence of 3 masses in pericardial space
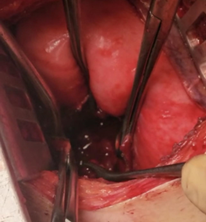
Figure 3: Tumor metastases in cardiac tissue
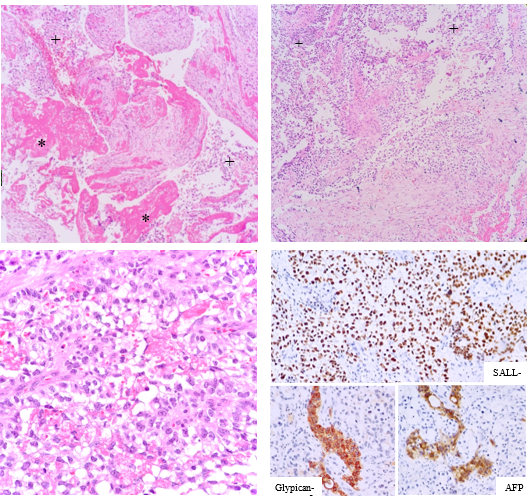
Figure 4: The slides show fragments of myocardium (*) with infiltration by cells with clear cytoplasm, nuclei of medium size and moderate atypia (+), alternating with areas of necrosis.
Testicular germ cancer is the most common solid malignancy in men between ages 15-35 years [9]. Histologically it is divided into two classes: seminomas and non-seminomatous tumor (NSGCT) [2]. In 40% of the cases diagnosed with non-seminomatous cell tumors, it is the most likely testicular cancer to cause metastasis, hematogenous metastases to the lung, bone, or brain may occur, but it metastasizes most frequently through the lymphatics to the retroperitoneum and may subsequently metastasize to contiguous mediastinal lymphatics [8,9]. One third of the patients with NSGCT are diagnosed with disseminated or metastatic presentations of the disease [2].
Intra-cardiac metastases are rare presentations of testicular germ cancer, but every cancer can spread to the heart [7]. Symptoms such as giddiness, fainting, fatigue, shortness of breath, chest discomfort and exertional fatigue are potential presentations in the emergency department on cardiac metastases, which are generic and non-specific [10]. Mediastinal metastases from NSGCT is mainly along the distribution of the thoracic duct and its major lymphatic tributaries, so it is very common to find metastases in the anterior mediastinal compartment or paravertebral sulcus and also middle mediastinal metastases [8].
Patients with NSGCT metastatic disease above the diaphragm are divided into low, intermediate, and high-risk groups, the risk stratification is based on their tumor markers level, histology, size of metastatic tumor, presence of cervical lymph nodes, and number of pulmonary metastasis, with a 5- year overall survival of 92%, 80% and 48% respectively [2]. All primary mediastinal non-seminomatous germ cell tumors are considered high risk and are pretty rare representing less than 10% of tumors among all cancer types when it’s an intracavitary presentation [2]. Treatment is based on cisplatin chemotherapy due to the high sensitive from nonseminomatous tumors, usually followed by surgery, most cases do not respond well to salvage chemotherapy [2,11]. Likewise, another indication of surgical treatment for NSGCT is the poor correlation between metastatic and primary testicular pathology; histopathologic discordance has been well-documented between testicular and mediastinal lesions [9]. Long term survival in such patients is < 10>
In the case of a primary extragonadal mediastinal and retroperitoneal non-seminomatous germ cell tumor like the one presented, a chemotherapy cycle is given with posterior resection of the primary tumor. [13] In the case of a metastatic disease the same approach should be given with cisplatin based chemotherapy to achieve citoreduction followed by resection of the remaining tumors, exactly as done with our patient [12,14].
In conclusion, metastatic cardiac non-seminomatous tumor is very uncommon and are of poor prognosis. The physician needs to be aware of this pathology during the differential diagnosis of a patient with non-seminomatous tumor for adequate therapeutic management.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
