
Case Report | DOI: https://doi.org/10.31579/2641-0419/006
1 Department of Cardiology, Ehime Niihama Prefectural Hospital, Tsukazaki Hospital.
*Corresponding Author: Shozo Sueda, The Department of Cardiology, Ehime Niihama Prefectural Hospital, Niihama City, Japan
Citation: Shozo Sueda, Hiroaki Kohno, Hirokazu Habara, Kaori Fujimoto, Acetylcholine spasm provocation test by trans-radial artery and vein approach: a case report. 1(2);DOI: 10.31579/2641-0419/006
Copyright: © 2018. Shozo Sueda. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 April 2019 | Accepted: 16 May 2018 | Published: 21 May 2018
Keywords: radial artery, radial vein, acetylcholine spasm provocation test.
70-year-old man admitted to our hospital because of chest discomfort on effort. Because we inserted the 6 Fr sheath into the wrong radial vein, we replaced the 5 Fr sheath into the radial vein. We inserted the 6 Fr sheath into the radial artery. We performed the acetylcholine and ergonovine spasm provocation tests under the temporary pace maker insertion. After the procedures, we compressed the radial artery and vein with radial band simultaneously. No bleeding or hematoma was found after the removal of radial band. We could perform the acetylcholine test via the radial artery and vein without any complications.
According to the Japanese Circulation Society (JCS) guidelines, the insertion of temporary pace maker is necessary during acetylcholine testing.1) We reported the brachial artery and vein approach spasm provocation tests of acetylcholine.2) We recently performed the radial artery and brachial vein approach spasm provocation test of acetylcholine. Here, we report a case whom we could successfully perform the acetylcholine test via the radial artery and vein approach procedure.
In 2000, 52-year-old man admitted to another hospital because of chest oppression on exercise. Just mild atherosclerosis on the mid left anterior descending (LAD) artery was found. Intracoronary ergonovine administration of 40 mg into the right coronary artery (RCA) caused focal spasm on segment 2-3, while subtotal occlusion at segment 7 was recognized after the administration of 64 mg ergonvoine into the left coronary artery (LCA). He was diagnosed as multiple coronary spastic angina. Under the two calcium-channel antagonists (nifedipine R 80 mg and benidipine 8 mg/day) and statin (fluvastatin 15 mg), he was well controlled. In 2018, coronary computed tomography was performed. Coronary atherosclerosis on both left anterior descending artery and circumflex artery was suspected, while myocardial thallium scintigraphy showed the anterior and inferior ischemia.
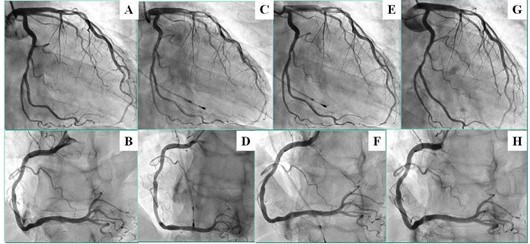
We tried to perform the coronary angiography including the acetylcholine test. We failed the puncture of brachial vein and punctured the radial artery. We inserted the 6 Fr sheath into the wrong radial vein. We replaced the 5 Fr sheath into the radial vein. We again punctured the radial artery near the radial vein and cannulated with 6 Fr sheath. (Figure 1-A) No significant coronary stenosis was found on control coronary angiography (Figure 2-A, 2-B). We performed the acetylcholine test on both coronary arteries (Figure 1-B). No spasm was provoked after the intracoronary administration of 20/50/80/100 mg acetylcholine (Figure 2-C, 2-D). Intracoronary ergonovine test was performed. Typical spasm was not provoked after the administration of 40/64 mg ergonovine (Figure 2-E, 2-F). After the administration of nitrate, no significant fixed stenosis was recognized (Figure 2-G, 2-H). We could successfully perform the pharmacological spasm provocation tests via the radial artery and vein approach procedures (Figure 1-C) and compressed the puncture sites with the radial band simultaneously (Figure 1-D). After the 8 hours’ compression of radial band, no bleeding or hematoma was found around the puncture sites. He discharged well next morning.

We could successfully perform the pharmacological spasm provocation tests including the intracoronary acetylcholine test via the radial artery and vein approach procedure. No bleeding or hematoma was found after the 8 hours’ compression of the radial band.
During performing the acetylcholine test, it is necessary to insert the temporary pace maker for safety. We used femoral vein, internal jugular vein, or brachial vein to insert the temporary pace maker. Initially, we performed the acetylcholine tests via the femoral artery and vein.3) Next, we performed the acetylcholine tests by the brachial artery and femoral vein. In 2000, we reported the brachial artery and vein approach acetylcholine tests. 1) Recently, we performed the radial artery and brachial vein approach acetylcholine tests. However, two compression sites were necessary and the exercise disturbance of the upper arm was recognized.
Acetylcholine testing without the temporary pace maker was reported by Ong et al. 4) However, even more than 3 minutes administration of acetylcholine showed the back-up pace maker rhythm set at 40 beats/minute in a quarter of patients with LCA testing. 5) Acetylcholine tests in the RCA were performed in just a third of their study patients. We recommend the temporary pace maker insertion when we performed the intracoronary acetylcholine testing as the JCS guidelines.
Although the routine radial vein insertion may be difficult, radial artery and vein approach acetylcholine tests were feasible and safe in this case. The most important issue was the just one compression site and more comfortable for patients.
We could successfully perform the radial artery and vein approach acetylcholine test without any complication in this case. When we failed the insertion of brachial vein sheath, radial vein insertion may be another choice on acetylcholine tests.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
