
Case Report | DOI: https://doi.org/10.31579/2690-8808/221
Bogomolets National Medical University, Kyiv, Ukraine.
*Corresponding Author: Yuliya V. Tyravska. Bogomolets National Medical University, Kyiv, Ukraine.
Citation: Yuliya V. Tyravska, Savchenko O. V. and Lizogub V.G. (2024), Case of Lambl’s excrescences and microthrombosis intracardially in young female with INOCA, J, Clinical Case Reports and Studies, 5(8); DOI:10.31579/2690-8808/221
Copyright: ©, 2024, Yuliya V. Tyravska. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 September 2024 | Accepted: 02 October 2024 | Published: 28 October 2024
Keywords: case report; Lambl’s excrescences; cardiac microthrombosis; INOCA; spontaneous echocardiographic contrast; blood viscosity
Ischemia and No Obstructive Coronary Artery Disease (INOCA) causes angina pectoris in 30-50% of young females leading to higher risk of major adverse cardiovascular events (death, non-fatal myocardial infarction, stroke), increased frequency of hospitalization, decreased quality of life and functional status. Missed diagnosis and mismanagement is rather typical of patients with INOCA. It can be provoked by mental stress, vasoconstriction, infections (including viral), vaccination, Lambl’s excrescences, which may lead to local blood rheology disorders and intracardial microthrombi formation. This paper reported the case of INOCA in a 28-year-old female patient with floating microthrombi in the left atrium, Lambl’s excrescences in the aorta, and reviews the relevant literature regarding above-mentioned disorders.
Angina pectoris (AP) in elderly patients is caused by stenosing atherosclerosis of the coronary arteries (CA), coronary spasm [1], and while its destabilization – predominantly by atherothrombosis [2]. Cardiac microvascular dysfunction (CMD) may aggravate the course of atherothrombosis [3]. Thus, the no-reflow phenomenon develops in 35% of patients with acute coronary syndrome after recanalization due to microembolization and thrombosis of myocardial microvessels, defective mitochondrial quality control. All these significantly impairs the effectiveness of recanalization and leads to the myocardial infarction [4].
Approximately 70% of patients with AP, particularly 30% of elderly patients, according to coronary angiography, have either hemodynamically insignificant atherosclerotic plaque in CA or absolutely no plaques are registered. Currently, this type of AP is defined as INOCA – ischemia and no obstructed CA [5]. The number of patients with intact CA at a young age is significantly higher in comparison with older one and is characterized by female preponderance, particularly it is established as a cause of AP in 30-50% of young females who undergo coronary angiography [6]. CMD plays a crucial role in INOCA occurrence, especially in women [5]. Traditional cardiac risk factors (smoking, arterial hypertension, hyperlipidemia, hyperglycemia and insulin resistance) as well as sex-specific factors (changes in blood estrogens level, autoimmune disorders, treatment for breast cancer) provoke INOCA occurrence [7]. Microvascular ischemia is tightly associated with endothelial dysfunction of arterioles [8]. Furthermore, psychological stress is a powerful trigger of vasomotor disorders and provokes so called mental stress-induced myocardial ischemia [9]. Recently, SARS-CoV-2 infection is found out to be additional factor that may aggravate endothelial dysfunction and as a result provoke or intensify microvascular ischemia [10]. Moreover, SARS-CoV-2 vaccines are disputable in terms of side effects and the influence onto microcirculation [11]. Thus, it is defined three endotypes of INOCA, particularly coronary microvascular dysfunction, epicardial coronary vasospasm and mixed one [12].
All over the above, local disorders of blood rheology, sometimes leading to intracardiac thrombosis with micro-embolization of the coronary microvasculature and the clinic of microvascular AP, as well as vasomotor disorders at a young age are not sufficiently investigated. Current clinical report presents the case of AP with local blood rheology disorders and microthrombosis intracardially in young female that arises the suspicions regarding INOCA.
Patient information
Female patient I., 28 years old, visited a cardiologist on an outpatient basis with complaints of recurrent episodes of stabbing pain in the heart region without a clear connection with physical activity without irradiation.
History of present illness
For the first-time paroxysmal pain with pressure in the heart region and behind the sternum, accompanied by shortness of breath, occurred 1 month before visiting the doctor. The attack was coped on its own, but since that time periodic stabbing pain has begun to disturb the patient. The first attack was associated with stress – death of the patient’s father.
Personal history
The patient had no history of any therapeutical disorders (including autoimmune diseases), surgeries, traumas, no harmful habits. Nothing remarkable in obstetric history was: no pregnancies, no history of miscarriage or spontaneous abortion. No allergic reactions were registered. The patient did not take any medications, including oral contraceptives. She was vaccinated against coronavirus twice (mRNA vaccine) 2 months prior to current episode of disorder manifestation.
Family history
The father's cause of death was pulmonary embolism. It has been known that for many years he was observed by a surgeon for chronic thrombophlebitis of the lower extremities. 6 months before his death, the diagnosis of permanent form of atrial fibrillation was established. One month later, he had a stroke for which he was hospitalized and was discharged in a relatively satisfactory condition. 3 weeks before the date of death, he was vaccinated with 1 dose of the vaccine against coronavirus (mRNA vaccine).
Clinical findings
Objectively: general condition of the patient was normal. She was normostenik, body mass index - 23.2 kg/m2. The skin and visible mucous membranes were clean. Blood pressure - 120/80 mm Hg, pulse 80 bpm, rhythmic. While physical examination no pathological changes were noticed in the internal organs.
Diagnostic assessment
On the ECG (Fig. 1), sinus regular rhythm was registered, negative T wave in lead III, no other peculiarities.
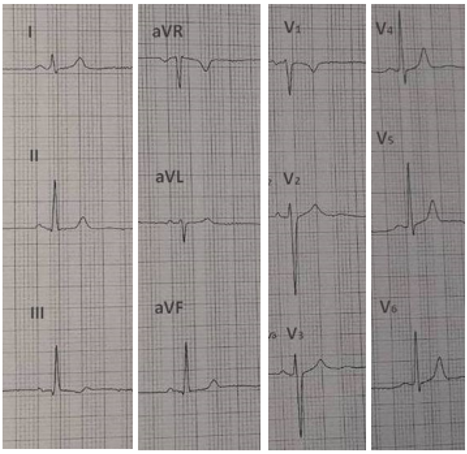

Figure 1: ECG of patient.
The patient underwent two-dimensional transthoracic echocardiography (Toshiba Artida, SSH-880CV). The heart volumes, wall thickness and ejection fraction (EF=65%) were normal.
However, an additional floating thread-like structure in aorta was noticed. We suspected it was Lambl’s excrescences which were attached to the non-coronarogenic aortic cusp. In the lumen of the aorta in the region of the right coronary cusp and the outflow tract of the left ventricle, we noticed the local areas of spontaneous echocardiographic contrast (local hemorheological changes). At the same time, larger areas of spontaneous echocardiographic contrast were registered in the region of the left atrium. Besides, a more echogenic and formed microthrombus on a thread (presumably fibrin) was attached to the anterior leaflet of the mitral valve. Though this microthrombus was localized in the left atrium, it passed through the mitral valve into the left ventricle and then returned to the left atrium. It resembled the effect of a tennis ball on a string (Figure.2).
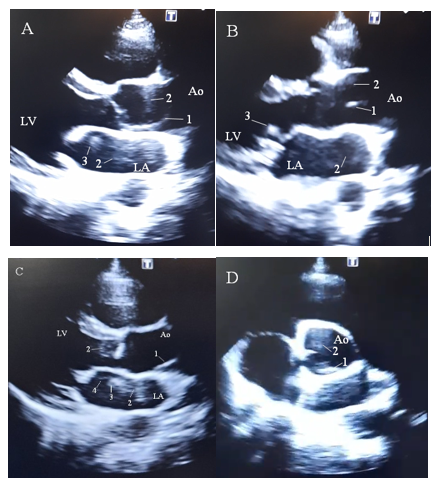
Figure 2: EchoCG of the patient: A, B, C - Parasternal long axis view; D – Apical short axis view; 1 – Lambl’s excrescences; 2 – phenomena of spontaneous echocardiographic contrast; 3 – microthrombus; 4 – thread of thrombus; LV – left ventricle, LA – left atrium, Ao – aorta.
Results of laboratory assessments have been aggregated in Table 1.
| Parameter | Result | Reference range |
| Complete blood count | ||
| Leukocytes, x109/L | 4.86 | 3.5-10.6 |
| Erythrocytes, x1012/L | 4.52 | 4.0-5.2 |
| Hemoglobin, g/L | 135 | 110-160 |
| Hematocrit, % | 42.8 | 35.0-47.0 |
| Mean corpuscular volume, fL | 94.7 | 75-98 |
| Mean corpuscular hemoglobin, pg | 29.9 | 27-34 |
| Mean corpuscular hemoglobin concentration, g/dL | 31.5 | 31.5-36.0 |
| Platelets, x109/L | 216 | 150-390 |
| Erythrocytes distribution width (RDW-SD) | 45.1 | 37-54 |
| Erythrocytes distribution width (RDW-CV) | 13.5 | 11-16 |
| Platelets distribution width, fL | 14.7 | 10-18 |
| Mean platelets volume, fL | 11.1* | 6.5-11 |
| Thrombocrit, % | 0.24 | 0.1-0.4 |
| Erythrocyte sedimentation rate, mm/h | 6 | < 15 |
| Blood differential test | ||
| Neutrophils, x109/L | 2.56 | 1.7-7 |
| Lymphocytes, x109/L | 1.92 | 1-4.8 |
| Monocytes, x109/L | 0.30 | 0-0.8 |
| Eosinophils, x109/L | 0.06 | 0-0.45 |
| Basophils, x109/L | 0.02 | 0-0.02 |
| Coagulogram | ||
| Prothrombin time, s | 11.6 | 9.8-12.5 |
| Prothrombin index, % | 88.4 | 70-130 |
| International normalization ratio | 1.10 | |
| Activated partially thromboplastin time, s | 30.2 | 22-32 |
| D-fibrinogen, g/L | 3.09 | 2-4 |
| Thrombin time, s | 19.6 | 14-21 |
| Closure time | ||
| Epinephrine/ Collagen, s | 152 | 84-160 |
| ADP/ Collagen, s | 88 | 68-121 |
| Lipidogram | ||
| Cholesterol, mmol/l | 4.86 | < 5.2 |
| Triglycerides, mmol/l | 0.48 | < 2.26 |
| High density lipoproteins, mmol/l | 2.4 | >1.68 – no risk (for females) |
| Low density lipoproteins, mmol/l | 2.67* | < 2.59 – optimal level |
| Very low density lipoproteins, mmol/l | 0.22* | 0.26-1.00 |
| Serum glucose, mmol/l | 4.81 | 4.11-5.89 |
Notes: * - out of reference ranges, ADP – adenosine diphosphate.
Table 1: Laboratory tests of the patient.
Diagnostic challenges. The patient had to go abroad in a few next days after visit. Consequently, the access to further profound investigational procedures was limited.
Diagnosis. We suspected AP caused by INOCA.
Therapeutic intervention
It was prescribed clopidogrel bisulfate 75 mg orally once a day and trimetazidine hydrochloride 35 mg MR twice a day.
Follow-up and outcomes
In 6 months, the patient had no possibility to visit the clinic to pass over the investigations (went abroad because of unforeseen circumstances). However, via cell phone call she mentioned about improvement in her condition (no pain in heart area, dyspnea or other unpleasant feelings) and well tolerated physical activity as well as emotional stresses.
It is well known that phenomenon of spontaneous echocardiographic contrast is observed mainly in patients with dilated heart cavities with a significant slowdown in blood flow velocity with low ejection fraction [13] or with atrial fibrillation, often in the left atrial appendage [14]. The effect itself is primarily associated with aggregation, erythrocytes agglutination and is one of the markers of the thrombi formation in the heart cavities [15].
However, according to the Virchow triad, in addition to the slow blood flow and its turbulence, the formation of a thrombus requires a violation of the vessel wall’s integrity (according to modern concepts, damage to the endothelium) and a violation of the blood rheological properties. The endothelium also lines the endocardium and the heart valves [16]. The coronavirus has a tropism for endothelial damage and microthrombosis [17]. Thus, according to autopsies of patients who died from coronavirus infection, endotheliocytes of small arteries and arterioles were located on the basement membrane unevenly in small groups or were single. For a long distance, the basement membrane remained bare, only individual cells retained their normal appearance. Most of the cells became rounded with light cytoplasm and prolapsed into the vessels’ lumen. Desquamated endothelial cells were also visualized. In places of cell desquamation, peri vassal erythrocytes’ aggregation and thrombus formation were detected [18]. The mechanisms of thrombus formation in COVID-19 continue to be studied but it was registered significantly greater fibrin and terminal complement C5b-9 [19].
Lambl’s excrescences on the cardiac valves during echocardiography have been registered for the last 15 years. The mechanism of their occurrence is still unknown. Presumably, these may be filaments of collagen and fibrin. These structures may result from damage to the valvular endothelium [20] and even are associated with acute myocardial infarction [21] or stroke [22] due to its embolization. As microthrombus is attached to the anterior leaflet of the mitral valve we suspect the damage of the valvular endothelium which can be among possible mechanisms of Lambl’s excrescences formation in current patient. Anyway, these findings highlight the increased risk of major adverse cardiovascular events in the patient. Further investigations are warranted to elucidate the association of these accessory structures on cardiac valves with immune-inflammatory processes in COVID-19.
Regarding erythrocytes sludge, that was manifested as local areas of phenomenon of spontaneous echo contrast in the aorta (the right and left CAs anatomically branch out from the aorta), as well as in the left atrium, it led to the formation of a mobile microthrombus. The phenomenon of local disorders in the blood rheological properties may be suspected. Erythrocytes aggregation coincides with an increase in blood viscosity leading to stasis [23]. The tissue or organ that is supplied with blood by these microvessels remains ischemic with all the ensuing consequences - hypoxia, acidosis, accumulation of metabolites, low-grade inflammation [24, 25, 26]. In the presented clinical episode, this is the microvasculature in the pool of the right CA.
The dependence of the blood plasma viscosity on the erythrocytes’ deformity has been established. The less erythrocytes membranes deformity, the greater blood viscosity [27]. The decrease in deformity may be due to an increase in the concentration of calcium ions in the erythrocyte membrane, which is observed, in particular, during hypoxia [28]. Viscosity becomes more pronounced with an increase in abnormal erythrocytes (for example, spherocytes) and erythrocytes containing an altered hemoglobin structure [27]. Besides, deviations in the deformity of erythrocyte membranes can change its electrical potential, which contributes to an increase in erythrocytes aggregation and a violation of the capillary’s spatial orientation [29]. Electrostatic forces and molecular bridges while rouleaux occurrence are considered as one of the leading aggregation mechanisms [30]. Blood viscosity depends on the protein and lipid plasma composition. An increase in the content of coarsely dispersed proteins in plasma leads to a blood viscosity enhancement. Thus, an increase in globulins up to 1-2% is accompanied by a doubling of viscosity. Thrombin and, especially, fibrinogen intensify blood viscosity (plasma viscosity is 20% higher than serum viscosity). The blood viscosity is increased by fibrinogen (fibrin) degradation products [31]. On the contrary, albumin leads to decrease in blood viscosity as an active antiplatelet agent [32]. The plasma lipid composition is of great importance. Blood viscosity intensifies with an increase in cholesterol / phospholipids ratio, low and very low density lipoproteins concentration, lipid peroxidation products [33]. Acidosis, in particular hypercapnia, also leads to blood hypercoagulability [25]. The slowdown in regional blood flow as a result of blood circulation centralization during stress is another factor causes widespread erythrocytes aggregation and sludge [34]. In the discussed particular clinical case, the patient had pain in the region of the heart after stress.
In complete blood count it was registered slightly increased mean platelets volume which is another marker of higher risk of cardiovascular events in patients as a sign of platelets activation triggered by endothelium dysfunction [35]. Several factors that can cause endothelium damage were found out in current patient, namely local blood rheology disorders, microthrombosis and Lambl’s excrescences. However, the platelets quantity and its aggregation quality were normal.
Among limitations of presented case report absence of appropriate follow-up should be mentioned. The monitoring of patient’s condition was provided only distantly via phone.
In the latest guides about INOCA management evidence-based data regarding treatment peculiarities for women are still absent [5]. However, according small sample-sized, short-term pilot studies of symptomatic women with INOCA, it is considered that statins in combination with angiotensin-converting enzyme inhibitor or receptor blockers improve angina, stress testing, myocardial perfusion, coronary endothelial function, and microvascular function [36].
The management of patients with enhanced blood viscosity is even less understandable. The principles for normalization of blood rheological properties should be based on [37, 38, 43]:
1. Normalization of hemodynamics (restoration of blood flow velocity);
2. Controlled hemodilution (blood thinning and viscosity reduction);
3. Antiplatelet agents and anticoagulants (prevention of thrombosis);
4. The usage of drugs that reduce the rigidity of erythrocyte membranes;
5. Normalization of the acid-base state of the blood;
6. Normalization of the protein composition of the blood (albumin solutions).
For the purpose of hemodilution and disaggregation of cells, hemodez and low molecular weight dextrans are used, which increase the electrostatic forces between blood cells due to an increase in the negative charge on their surface, lower blood viscosity by attracting water into the vessels, cover the endothelium and vessels with a separating membrane, form complex compounds with fibrinogen, reduce the lipids concentration [44].
In young patients, cardialgia may be caused by either microvascular ischemia due to local disturbance of blood rheology with the formation of intracardiac thrombi or vasospasm caused by mental stress. Physicians should take into account INOCA as one of possible differential diagnosis in young females with chest pain and cardiovascular risk factors.
The hand-written informed consent of the patient was obtained after detailed explanation of the purpose of the investigations. The patient was managed according to the ECS guidelines. The lack of some investigations is due to local specificity. Nonessential identifying details are omitted. The identifying characteristics of the patient are deidentified without distorting of the scientific meaning.
We are highly thankful the nurse Yuliia Sivtsova for assistance in data collection.
No AI-assisted technologies
No Financial, non-financial relationships and activities are declared
No conflicts of interest are declared.
Oleksandr Savchenko – conception and design of the case, acquisition of data, analysis and interpretation of data, critical revising, final approval;
Yuliya Tyravska – concept and design of the study, analysis and interpretation of data, drafting the article, critical revising, final approval;
Tarana Nadeem – acquisition of data, critical revising, final approval;
Viktor Lizogub – critical revising, final approval.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
