
Research Article | DOI: https://doi.org/10.31579/2692-9759/005
*Corresponding Author: Momar Dioum. Cardiology department, Fann Hospital, Faculty of Medicine, Pharmacy and Stomatology, University Cheikh Anta Diop of Dakar (Senegal) ; Cheikh Anta DIOP avenue PO Box : 5035.
Citation: Dioum M, Issa KA, Joseph S Mingou, Papa N Ndiaye, Fatou Aw. (2020) Care time Delays in Acute Coronary Syndromes with Persistent St Elevation (stem) and the Delaying Factors: Prospective STUDY About 50 Cases in the Cardiology Department of Aristide le Dante Hospital. Cardiology Research and Reports, 2(1): Doi: 10.31579/2692-9759/005
Copyright: © 2020. : Momar Dioum. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 March 2020 | Accepted: 06 March 2020 | Published: 15 March 2020
Keywords: STEMI; delays; PCI; fibrinolysis; dakar
The care of acute coronary syndrome with persistent ST-elevation (STEMI) is a time-trial race: ‘‘time is myocardium”. The treatment relies on myocardial reperfusion by percutaneous coronary intervention (PCI) or fibrinolysis as promptly as possible. The main objective of this work was to assess the care time delays and the delaying factors during STEMI.
We conducted a prospective, descriptive and analytic study over a 6 months’ time period. Were included all the patients received for
STEMI. We have studied the care time delays and the delaying factors.
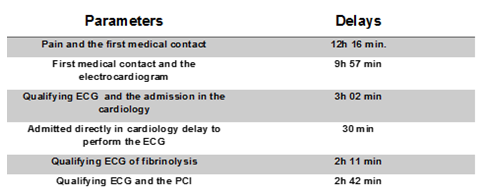
We have compiled 50 patients. The mean age was 58.4 years and the sex-ratio M/F 2.5. The chest pain was typical in 39 patients. The mean time elapsed between the beginning of the pain and the first medical contact was 12 h 16 min. Transport (76%) and self-medication (70%) were the significant delaying factors found (p = 0.0001). The mean time elapsed between the first medical contact and the electrocardiogram was 9 h 57 min. The main factors delaying the diagnosis were the unavailability of the electrocardiogram device and the absence of electrocardiogram prescription (p = 0.001). The mean time elapsed between the electrocardiogram and the admission in the cardiology department was 3 h 02 min. The transport was the principal factor lengthening that time delay (p = 0.0001).
Among the patients admitted directly in cardiology department, the mean time delay to perform the ECG was 30 min. The mean time delay of fibrinolysis was 2 h 11 min. Streptokinase shortage was the most frequent delaying factor (p = 0.001). The mean time delay between the qualifying ECG and the PCI completion was 2 h 42 min. The unavailability of the medical team was the first factor lengthening that time delay (p = 0.0001).
The care time delays were lengthened enough in our context. This testifies to the lack of a codified strategy for STEMI care. It is essential to develop pre-hospital emergency medicine and sensitize the population and healthcare professionals.
Coronary artery disease has known a regular progression in Senegal with the westernization of the lifestyle and the influence of cardiovascular risk factors. The hospital prevalence of acute coronary syndrome (ACS) went from 7.61% in 2009 to 10% in 2016 [1].
Myocardial infarction represents the most severe form of this pathology. The myocardial reperfusion by percutaneous coronary intervention (PCI) or fibrinolysis represent the cornerstone of the treatment [2].
The promptness and efficiency of this reperfusion are the 2 factors that condition the morbidity and mortality rates in the short and long term. The challenge is then to re-canalize the culprit artery and reperfuse the myocardium as soon as possible [3]. The ESC guidelines [4] stipulate that it should be done within 120 minutes maximum following the first medical contact.
There are many steps in STEMI care. Many time delays have been used in the English literature: time-to-first call, symptom onset-to-door, door-to-balloon, time to reperfusion. The European Society of Cardiology has proposed the notion of “first medical contact” (FMC), defined by “the place (ambulance or hospital) where, at least in principle, the reperfusion treatment could be initiated”.
According to the ESC guidelines of 2017 [4], every patient with STEMI must receive a reperfusion strategy in the 12 first hours following the symptoms. However, in sub-Saharan Africa and especially in Senegal, because of the lack of appropriate organization, the patients attend healthcare beyond the twelfth hour [5].
Thus, our study has focused essentially on the analysis of the admission and care time delays of STEMI admitted in the Cardiology Department of Aristide Le Dantec Teaching Hospital.
The specific objectives were to:
Methodology
It was a prospective, descriptive and analytic study over 06 months (March 1st to September 30th, 2018). Were included, after informed consent, all the patients received for a STEMI during the study period.
We have assessed the time delays at different levels:
The factors lengthening these time delays have been analyzed as well as the clinical, electric and angiographic data.
The data were input in EXCEL® software version 2007. The data analysis has been made with SPSS software version 20.
we have compiled 50 patients. The mean age was 58.4 years (40 – 88 years). The population was made mostly of men with a sex ratio M/F of 2.5. Arterial hypertension was in the forefront of the cardiovascular risk factors found with a 46% prevalence.
The chest pain was typical in 39 patients. The majority of patients (n = 40; 80%) was referred to the cardiology department mostly via healthcare facilities (29 patients, or 58%). Ten patients or 20% were admitted directly in cardiology. The initial treatment was made of proton pump inhibitor (62%), analgesic (60%) and antacid (54%). Aspirin and Clopidogrel were prescribed respectively to 34% and 20% of the patients. More than the half of the patients (n = 29) did not know the existence of pre-hospital facilities. Private car and taxi were the most used mean of transport by our patients to attend the cardiology department. The mean time delay between the pain onset and the first medical contact was 12 h 16 min with extremes of 15 min and 07 days. The 1st medical contact was the general practitioner in 33 patients; followed by the cardiologist (n = 8) and the nurse (n = 6). Transport (76%) and self-medication (70%) were the most significant lengthening factors found (p = 0, 0001). The mean time delay between the first medical contact and the ECG completion was 9 h 57 min (5 min and 07 days). The main factors delaying the diagnosis were the unavailability of the ECG device and the absence of ECG prescription (p = 0.001). The mean time delay between the ECG completion and the admission in the cardiology department was 3 h 02 min with extremes of 30 min and 48h. Transport was the main factor lengthening that time-delay (p = 0.0001) followed by financial issues. Among the patients directly admitted in cardiology, the mean time delay to perform ECG was 30 min (02 – 120 min). The slowness of the paramedical personnel was the main delaying factor (64%) with a significant p of 0.0001. Thirty-five (35) patients were admitted on time for the fibrinolysis. Seventeen patients or 34% has benefit from fibrinolysis. The mean time delay for fibrinolysis was 2 h 11 min with extremes of 40 min and 7 h. A shortage of streptokinase was the most frequent delaying factor (p = 0,001). A primary PCI was performed in 23 patients with a mean time delay of 2 h 42 min with extremes of 30 min and 10h between the qualifying electrocardiogram and the transfer to the coronary angiography room. The unavailability of the medical or paramedical team was the factor lengthening that time delay (p = 0.0001).
In our series, we have noticed a male predominance (72%). This result is comparable to the literature in Africa (INTERHEART Africa) [6] and in the West [7]. This difference between the two genders could be explained by the protective effect of estrogen in women before menopause. Our patients were one-decade younger compared to western series [8, 7, 9].
In Africa, especially Saharan, patients attend generally peripheral healthcare facilities before being referred to cardiology. Yameogo [5] in Burkina has found 3 facilities attended before admission in cardiology. Thus, the general practitioner was the firstt medical contact in 33 patients (64%). Only eight patients have been consulted by a cardiologist (16%). This could be explained by the health pyramid, the proximity of the districts and the low cost of care.
Private car and taxi are the means of transport mostly used by our patients (54%) to attend the cardiology department. It is the general rule in Africa [5, 10]. The pre-hospital facilities are exceptionally requested. This strategy differs from European countries, where the emergency rapid respond units are very requested [11]. However, the high cost of these services and their availability could be an obstacle for their use. The means of transport used by the patients compete to lengthen the admission time delays. As found in the other African studies [5, 12], the mean time delay between the pain onset and the consultation was 12h 16min. The delaying factors were transport and self-medication. The mean time delay between the first medical contact and the completion of electrocardiogram was 9h 57 min for out-care patients. It was 39.77 min for patients admitted directly in cardiology. This is far from ESC 2017 recommendations that require a time delay of 10 min [4] to perform a 12-lead ECG when a patient is cared for chest pain. The factors responsible for this long time delay were the ignorance of the medical contact, the impossibility to perform ECG and the paramedical slowness. Out-care patients diagnosed were admitted after 3 hours because of transport or financial issues, or ECG interpretation. The mean time delay to start the fibrinolysis was long (130.53 min) compared to YAMEOGO (34 min) [5], and Hadj (122 min) [12]. The shortage of streptokinase was the delaying factor mostly noticed. Thus, the mean time delay (2.7 h) to perform primary PCI was better than Hadj’s (6h 28min) [12]. The unavailability of the medical team was the most noticed lengthening factor.

The care time delays were quite lengthened in our context. This shows the lack of codified care strategy of STEMI. It is essential to develop pre-hospital emergency medicine and sensitize the population and healthcare professionals.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‚Äëfree, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
