
Case Report | DOI: https://doi.org/10.31579/2641-0419/461
1Professor, Shupyk National Healthcare University of Ukraine, 04107, Kyiv.
2Shupyk National Healthcare University of Ukraine, 04107, Kyiv.
3Associate professor, P.L. Shupyk National Healthcare University of Ukraine; 04107, Kyiv.
*Corresponding Author: Golyanovskiy Oleg V, Professor, Shupyk National Healthcare University of Ukraine, 04107, Kyiv.
Citation: Golyanovskiy Oleg V, Vorona Roman М, Ostrovets Kateryna S, Voloshyn Oleksandr A, Fedorenko Dmitro S., (2025), Cardiometabolic Disorders in A Pregnant Woman with Severe Preeclampsia on the Background of Morbid Obesity (Case Report), J Clinical Cardiology and Cardiovascular Interventions, 8(5); DOI: 10.31579/2641-0419/461
Copyright: © 2025, Golyanovskiy Oleg V. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 March 2025 | Accepted: 20 March 2025 | Published: 31 March 2025
Keywords: morbid obesity; cardiometabolic disorders; cesarean section; supraumbilical laparotomy; fundal cesarean section; preeclampsia;postpartum hemorrhage
The World Obesity Federation predicts that by 2030, one billion people worldwide will be living with obesity. Therefore, it is worth highlighting morbid obesity, defined by the WHO as a BMI of 40 kg/m2 or more, in which women have significantly more prenatal, perinatal, and postpartum complications. In particular, obesity is known to have a significant association with cardiometabolic disorders. Іt has been established that the rate of cesarean section (CS) in pregnant women with a BMI ≥ 50 kg/m2 approaches 50%. The purpose of the publication is to familiarize with a clinical case of cardiometabolic disorders and the optimal method of delivery of a pregnant woman with morbid obesity and severe preeclampsia using supraumbilical laparotomy and fundal CS, medical and technical support with modern energies (radio-wave scalpel, argon-plasma tissue coagulation) for the prevention of peripartum complications, and which was carried out at the main clinical base of the department - the Kyiv Regional Perinatal Center (KRPC).
Having analyzed the clinical case we successfully conducted, it is worth highlighting the timely diagnosis of cardiometabolic disorders in a pregnant woman against the background of morbid obesity and severe preeclampsia with all the obvious advantages of supraumbilical/supraumbilical laparotomy and fundal CS, which is most effectiveness for this contingent of women.
Obesity is a serious public health problem in the modern world. The World Health Organization (WHO) characterizes obesity as a complex chronic disease in which excessive accumulation of adipose tissue can negatively affect human health [1, 2].
Obesity contributes to dysfunction of various organs and body systems, creating prerequisites for the development of extragenital diseases and reduced resistance to infection, which increases the risk of pathological course of pregnancy, childbirth, postpartum period in women, and perinatal morbidity and mortality in newborns [3,4].
Moreover, women with morbid obesity have a high frequency of menstrual dysfunction, which may indicate a close relationship between obesity and the development of dyshormonal changes in the female reproductive system, infertility, and miscarriage [5].
The prevalence of obesity is steadily growing, demonstrating a global problem at the pandemic level. According to WHO, about 16% of adults worldwide aged 18 and over suffer from obesity as of 2022. From 1990 to 2022, the prevalence of obesity worldwide has more than doubled [1].
It is estimated that around 39 million pregnancies worldwide are annually complicated by obesity in mothers, and in some countries, the prevalence of overweight and obesity during pregnancy exceeds 60% (South Africa 64%, Mexico 65%, USA 55-63%) [6, 7]. In the United Kingdom, it was estimated that approximately 1 case out of 1000 births occurs in women with BMI > 50 kg/m², while in Australia, the prevalence of excessive obesity was noted at 2.1 per 1000 births [6].
Although overweight and obesity significantly increase the risk of adverse outcomes during pregnancy, it is important to understand that most women with BMI > 25 kg/m² will have a normal, uncomplicated pregnancy [6]. Therefore, it is worth highlighting morbid obesity, defined by WHO as BMI of 40 kg/m² or more, in which women are significantly more prone to developing cardiometabolic problems, antepartum, perinatal, and postpartum complications [8].
Among antepartum complications, the most common are cardiometabolic disorders, premature birth, and urgent cesarean section (CS) [9, 10]. Cardiometabolic diseases represent a complex phenotype of cardiovascular and metabolic dysfunction characterized by insulin resistance and impaired glucose tolerance, dyslipidemia and obesity, hypertension, and cardiovascular diseases (CVD) [29]. Additionally, pregnancy with morbid obesity has an increased risk of stillbirth [11].
Preeclampsia is a major cause of premature birth because the main treatment for this condition is delivery by cesarean section (CS). According to a systematic review of 13 cohort studies involving nearly 1.4 million women, the risk of preeclampsia doubles for every 5-7 kg/m² above the ideal BMI [12].
Women with gestational arterial hypertension have a higher risk of subsequently developing chronic arterial hypertension (CAH), cardiovascular diseases, coronary heart disease, myocardial infarction, heart failure, ischemic cerebrovascular disease, chronic kidney disease, and diabetes mellitus outside of pregnancy in the future [28].
Women with obesity have an increased risk of developing metabolic syndrome (MS). According to various authors, the prevalence of MS continues to increase and currently ranges from 5 to 20% [13]. Increased insulin resistance during pregnancy can cause existing but subclinical cardiometabolic dysfunction, which in turn manifests as preeclampsia, gestational diabetes, and obstructive sleep apnea (OSA). These complications are associated with adverse pregnancy outcomes. Compared to women without OSA, women with this pathology more often suffer from preeclampsia, eclampsia, cardiomyopathy, pulmonary embolism, and hospital mortality [11]. If the result of primary early diabetes screening is negative, repeat diabetes screening is usually performed at 24-28 weeks of pregnancy [11].
The connection between obesity and increased risk of CS is well demonstrated, as the frequency of CS in patients with BMI ≥ 50 kg/m² approaches 50% [8]. According to research results, this is because women with morbid obesity much more often than women with obesity have preeclampsia and fetal macrosomia [14, 15]. Many studies have shown a linear correlation between maternal pre-pregnancy BMI and newborn weight [15]. Data from prospective cohort studies have shown that normalizing body weight in women with obesity reduces the risk of giving birth to a large baby [12]. Also, research results indicate a negative impact of the type of adipose tissue distribution on the degree of cervical maturity, timely onset of labor, and its nature [16].
It is reported that the frequency of urgent CS in women with pathological obesity ranges from 42 to 50% compared to approximately 9% in the control group [15]. Maternal obesity is also associated with prolonged surgical intervention time. Pregnant women with obesity, during repeat delivery after a previous CS, have almost twice the cumulative maternal morbidity and a five-fold risk of neonatal injury [11].
After CS, women with obesity have more postoperative complications compared to patients without obesity, including: postpartum hemorrhage (34.9% of patients with massive obesity versus 9.3% of women without obesity), peritonitis, endometritis (32.6% for patients with massive obesity versus 4.9% in other cases), wound infection, and venous thromboembolism [14].
Postpartum hemorrhage (PPH) is an emergency obstetric complication that accompanies 1-10% of all births. It is defined as a quantitatively expressed bleeding volume of more than 500 ml during vaginal delivery and more than 1000 ml during CS, occurring within the first 24 hours after delivery [17, 18]. Obesity is one of the key risk factors for postpartum hemorrhage. Thies-Lagergren L. et al. reviewed data on more than 400,000 pregnancies in the Swedish Birth Registry. A greater risk of blood loss exceeding 1000.0 ml within 2 hours after birth was observed in women with BMI > 25 kg/m² [19].
The purpose of the publication is to familiarize with a clinical case of cardiometabolic disorders and the optimal method of delivery for a pregnant woman with morbid obesity and severe preeclampsia using supraumbilical laparotomy and fundal CS, medicinal and technical support with modern energies: radio-wave (RW) scalpel, argon-plasma tissue coagulation (APC) for the prevention of peripartum complications, which was conducted at the main clinical base of the department - Kyiv Regional Perinatal Center (KRPC).
Pregnant woman L., 30 years old, was urgently hospitalized to KRPC on referral from one of the districts of Kyiv region at the term of her first pregnancy 36-37 weeks with complaints of shortness of breath when walking, swelling of the lower extremities and anterior abdominal wall.
According to her history, over the past 4 years, she has noted periodic increases in blood pressure (BP) to 190/110 mm Hg; she was monitored for chronic arterial hypertension (CAH) at her place of residence. At the admission department, she was examined by the on-duty team of obstetricians-gynecologists, a therapist, and an ophthalmologist.
Upon examination, significantly increased body weight is notable, BMI - 61.2 kg/m², which corresponds to morbid obesity, pronounced edema of the lower extremities and anterior abdominal wall, shortness of breath. BP - 170/100 mm Hg, pulse (Ps) - 100 beats/min. The abdomen is enlarged by the pregnant uterus to 36-37 weeks, the height of the uterine fundus is 37 cm. A transverse position of the fetus, II position is determined; the fetal heartbeat is clear and rhythmic at the level of the navel - 144 beats/min.
A preliminary diagnosis was made: Pregnancy Ist, 36-37 weeks. Transverse position of the fetus, II position. CAH grade II with combined preeclampsia. Heart failure (HF) 0. Angiopathy of the retina of both eyes. Sinus tachycardia. Gestational hypothyroidism (medically compensated - daily oral intake of 50 μg Euthyrox). Morbid obesity. BMI - 61.2. Metabolic syndrome.
Given the CAH II, combined preeclampsia, and morbid obesity, she was hospitalized in the Department of Anesthesiology and Intensive Care (DAIC) of KRPC. A complete clinical and laboratory examination, ultrasound examination of the fetus and the pregnant woman's heart (echocardiography), and cardiotocographic examination were ordered. Comprehensive therapy for CAH and combined preeclampsia was prescribed according to the Order of the Ministry of Health of Ukraine No. 151 dated January 24, 2022 [20].
According to fetal ultrasound data: pregnancy 37 weeks, transverse position of the fetus, II position, according to fetometry, the expected fetal weight is 4000.0±200.0 g. Placenta on the anterior wall of the uterus, II degree of maturity, thickness 39 mm. Amniotic index - 177 mm, Doppler measurements in the vessels of the umbilical cord and middle cerebral artery - without pathological changes. Systolic-diastolic ratio - 1.55. The cervix is formed, length 3 cm, internal os is closed.
Despite intensive monitoring and therapy in the DAIC for three days, the pregnant woman's condition deteriorated due to the appearance of generalized edema, unstable hemodynamics (refractory arterial hypertension that did not respond to medication), pulse - 110 beats/min, signs of tachypnea (respiratory rate = 28/min), clinical signs of heart failure (hydropericardium), as well as laboratory indicators confirming the progression of preeclampsia (proteinuria - 3.3 g/l, total protein - 53 g/l, BP - 160/110 mm Hg).
Pre-operatively, an assessment of the risk of venous thromboembolic complications in obstetrics was conducted (according to the scale adapted from RCOG Green-top Guideline No. 37a. 2015), according to which the patient received 3 points, identified as a high level of risk for thromboembolic complications. In connection with this, in the postpartum period up to 6 weeks, the use of compression stockings on the lower extremities, early activation, and a high prophylactic dose of low molecular weight heparins (LMWH) are indicated (according to the pregnant woman's body weight - Enoxaparin 80 mg per day up to six weeks postpartum).
Due to the lack of clinical effect from comprehensive therapy for combined preeclampsia, deterioration of the pregnant woman's general condition, and considering the data obtained from additional examinations (presence of hydropericardium, presence of fluid in the pleural cavity), mitral valve insufficiency grade I, HF II, a consilium was held to determine further management tactics for the pregnant woman, the method and facility for delivery, consisting of the head of the Department of Obstetrics and Gynecology No. 1 of the P.L. Shupyk National University of Health Care of Ukraine, the medical director of KRPC, department heads, and specialist consultants (M. Amosov National Institute of Cardiovascular Surgery, O. Lukyanova State Institution "All-Ukrainian Center for Motherhood and Childhood of the National Academy of Medical Sciences of Ukraine").
The consilium established the diagnosis: Pregnancy I, 37 weeks. Transverse position of the fetus. Severe preeclampsia against the background of CAH stage II, grade 2. Heart failure I. Functional class III, with preserved left ventricular ejection fraction. Mitral valve insufficiency grade I. Angiopathy of the retina of both eyes. Morbid obesity (BMI - 61.2 kg/m²), cardiometabolic syndrome. Gestational hypothyroidism (medically compensated).
The consilium reached a consensus that the signs of heart failure, presence of hydropericardium, fluid in the pleural cavity are associated with generalized edema against the background of severe combined preeclampsia in a pregnant woman with morbid obesity and cardiometabolic disorders.
Considering the severe preeclampsia against the background of CAH (clinical and laboratory: protein in 24-hour urine 3.3 g/l, total blood protein 53 g/l, albumin 30 g/l; objectively: generalized indurative edema with skin peeling and itching, shortness of breath at rest - respiratory rate 25/min), as well as the transverse position of the fetus according to ultrasound data, according to the consilium's decision, urgent delivery of the pregnant woman by CS operation at KRPC is indicated. Informed consent from the patient for surgical intervention was obtained. The patient was informed about the possible extension of the surgical intervention and the need for transfusion of blood products, and consent was obtained.
Various surgical options for the incision of the anterior abdominal wall and CS were considered by the operating team and discussed with the pregnant woman, but given the pronounced indurative edema of the apron-like panniculus (Figure. 1, 2), lack of possibility for its retraction/displacement and, as a result, the impossibility of performing laparotomy in the lower abdomen (below the navel), it was decided to perform supraumbilical (upper-middle) laparotomy with CS in the uterine fundus (fundal CS).
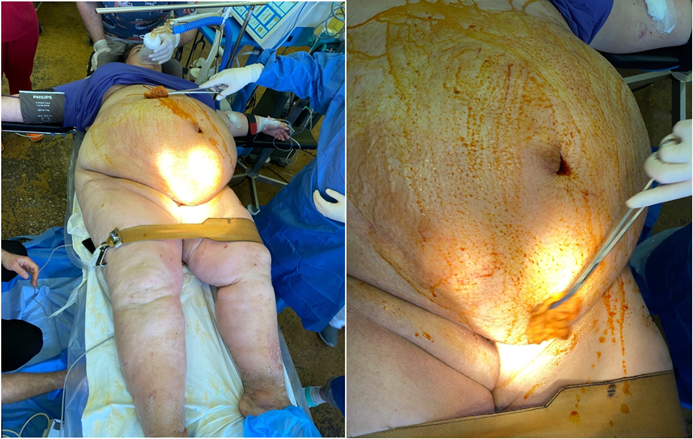
Figure. 1,2: Pregnant woman L., with morbid obesity, generalized edema against the background of severe combined preeclampsia and indurative edema of the panniculus, which made access to the lower segment of the uterus impossible.
Features of the CS operation. Under spinal analgesia, a supraumbilical (above the navel) incision of the anterior abdominal wall (upper midline laparotomy) was performed - Figure. 3.
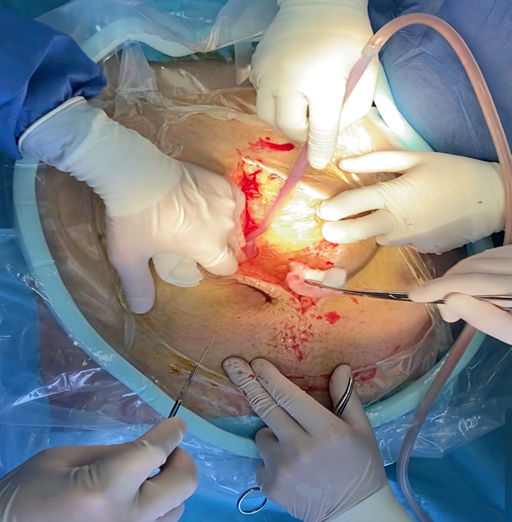
Figure 3: Supraumbilical longitudinal incision of the anterior abdominal wall during fundal CS in a pregnant woman with morbid obesity.
During the laparotomy, edema of the subcutaneous fatty tissue was notable, with a thickness of about 12 cm. In the abdominal cavity, there was up to 1.5 liters of transudate (Rivalta test negative). A fundal cesarean section was performed. A live full-term baby girl was delivered by the pelvic end, weighing 3900 g, 56 cm in height, with 7/7 Apgar scores; delayed umbilical cord cutting (2nd minute), the newborn was transferred to the care of a neonatologist. The uterus was sutured with a double-row continuous Vicryl suture. Given the high risk of hemorrhagic complications, to prevent postpartum post-operative bleeding, 100 μg of carbetocin was administered intravenously slowly, tranexamic acid - 1.0 g; a polyvinyl chloride (PVC) drain with a diameter of 15 mm was inserted into the uterus using the "lower uterine segment remodulation" ("RENIS") technique [21]. The uterus contracted.
During the operation, a monopolar RW-scalpel and APC were also used to reduce blood loss. Layered laparorrhaphy was performed. Drainage of the abdominal cavity and subcutaneous fatty tissue with active PVC drains 1.0 cm in diameter. Total blood loss was 570.0 ml. Urine through catheter - 170.0 ml (clear). Given the volume of intraoperative blood loss, there was no need for transfusion therapy.
The course of the postoperative period was without complications, with positive clinical dynamics of preeclampsia therapy: stabilization of blood pressure at 140/90, absence of shortness of breath (respiratory rate - 16/min), progressive reduction of edema and proteinuria. Prevention of purulent-inflammatory complications was carried out according to generally accepted standards (Cefazolin 1000 mg intravenously as a one-time infusion 30 minutes before the start of surgery) with continued antibiotic therapy according to the Order of the Ministry of Health of Ukraine No. 8 dated January 5, 2022 [22]. Given the high risk of thromboembolic complications, she received LMWH (enoxaparin 80 mg per day, subcutaneously) [22]. Drains were removed on the 4th day of the postoperative period. Results of laboratory tests on the 3rd day after CS:
Ultrasound data: The uterus has normal echo-structure, dimensions 127*99*85 mm. The uterine cavity is not enlarged. Sutures are visualized in the area of the uterine fundus, without peculiarities. No free fluid in the abdominal cavity was detected. Uterine appendages are not visualized. The bladder has clear contours, without peculiarities. Normal uterine involution as of the 5th day after the fundal cesarean section.
During the first 3 days of the postoperative period, she was in the DAIC, where intensive observation and comprehensive therapy of severe combined preeclampsia were conducted, and from the 4th day, she was transferred to the postpartum department for joint stay with the child. In the postoperative period, there was not a single day of hyperthermia or inflammatory changes in the postoperative wound (Fig. 4). On the 8th day after CS, sutures were removed from the anterior abdominal wall, healing of the postoperative wound was per primam (primary intention).

Figure 4: Healing of the postoperative wound on the 8th day after CS per primam.
On the 9th day after CS, the woman and her newborn were discharged in satisfactory condition to their place of residence under the supervision of a district obstetrician-gynecologist, neonatologist, and family doctor. Recommendations were provided regarding monitoring and therapy for CAH, morbid obesity and body weight correction, postpartum hygiene, contraception, and planning the next pregnancy no earlier than 2 years after CS. The woman was warned about the need to continue prevention of thromboembolic complications on an outpatient basis with LMWH medications (enoxaparin - 80 mg) and wearing compression stockings for up to 6 weeks from the day of CS, which was also communicated by phone to the obstetrician-gynecologist at the woman's place of residence [22].
Patients with morbid obesity have a higher level of cardiometabolic and surgical problems, namely: increased duration of surgery, amount of blood loss, higher doses of neuraxial anesthesia, and a significantly higher need for general anesthesia; postpartum women more often develop purulent-inflammatory complications (endometritis, wound infection), postpartum hemorrhage, and thromboembolic complications [14].
When performing delivery by CS, laparotomy is usually performed using the Joel-Cohen or Pfannenstiel techniques. These are low transverse suprapubic approaches, the advantages of which are cosmetic appearance, moderate postoperative pain, quick healing period, and minimal blood loss. However, when considering the use of these incisions in patients with obesity, significant technical obstacles arise during CS, due to difficult retraction of subcutaneous fatty tissue, which significantly reduces the field of view of the surgical site [15]. We also absolutely agree with opinion of this authors.
Some authors consider the supraumbilical incision of the anterior abdominal wall to be the optimal alternative laparotomy option in women with morbid obesity, which avoids placing the wound under the "apron" - panniculus [15, 23].
The principle of this laparotomy is to improve access to the fundus and body of the uterus. It is worth noting that since the panniculus is voluminous, it is difficult to find anatomical landmarks. Above the navel, the thickness of the fat layer is minimal, which facilitates access to the uterus, simplifies extraction of the fetus, and reduces the risk of parietal complications [9, 24].
Usually, when using an upper-midline/supraumbilical incision, access to the lower segment of the uterus worsens, so the probability of performing corporal or fundal CS increases. This helps reduce the volume of blood loss, as the muscle layer of the uterine fundus is thinner than the myometrium of the uterine body, and the incision is performed parallel to the course of the arcuate arteries [15, 25]. In our mind supraumbilical laparotomy is most effective method for delivery woman with morbid obesity. Performed this case we saw the advantages of sumpraumbilicallaparotomy and fundal CS which also characterized by strong uterine contractions after placental birth, which suppress bleeding from the site of the detached placenta without the need for additional compressive hemostatic sutures [15, 25].
Analyzing our successfully conducted clinical case, it's worth highlighting the timely diagnosis of cardiometabolic syndrome and severe combined preeclampsia against the background of morbid obesity and CAH, and all the obvious advantages of supraumbilical laparotomy and fundal CS in pregnant women with morbid obesity, namely: optimal access to the fundus and body of the uterus, convenience of fetal extraction, reduction of blood loss and postoperative pain, rapid recovery after surgery, early restoration of intestinal peristalsis, possibility of early mobilization, and reduced hospital stay. Our clinical case results are consistent with the limited scientific literature data on this issue [10, 23, 26].
The following criteria for the condition of the postoperative scar on the uterus can provide a safer subsequent pregnancy: absence of a "niche" in the area of the uterine scar, scar thickness index ≥ 70%, normal blood flow in the uterus according to color Doppler mapping, and absence of anomalies on sonohysterogram [23, 25, 27].
The presented clinical case of morbid obesity, metabolic syndrome, and CAH, which led to the development of severe combined preeclampsia during pregnancy, cardiometabolic dysfunction, and signs of heart failure, became an indication for urgent delivery by CS.
In this context, it is worth highlighting all the obvious advantages of supraumbilical laparotomy and fundal CS in pregnant women with morbid obesity: optimal access to the fundus and body of the uterus, convenience of fetal extraction, reduction of blood loss and postoperative pain, probability of developing purulent-inflammatory postpartum complications, rapid repair of the postoperative wound, and reduced hospital stay.
The use of modern medication support (carbetocin, tranexamic acid), technical support (radio-wave scalpel, argon-plasma tissue coagulation) during CS, drainage of the abdominal cavity and subcutaneous fatty tissue, and the use of low-molecular-weight heparins in this contingent of pregnant women minimize postoperative complications.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
