
Review Article | DOI: https://doi.org/10.31579/2641-0419/358
1The Russian Academy of Natural Sciences (RANS), Moscow, Russia.
2Dept for Clinical Allergology & Immunology of the Russian University of Medicine, Moscow, Russia.
3EPMA, Brussels, EU.
4PMC, Washington, DC, USA.
5ISPM, Tokyo, Japan.
6AHA, Houston, TX, USA.
7Department of Neurophysiology of Kazan State Medical Academy, Kazan, Russia.
8New York Academy of Sciences, USA
9Faculty of Medicine and Life Sciences, University of Hasselt, Belgium.
10Stem Cell Biology Lab, Department of Medicine, Cardiology Division, UCSF, S-F, CA, USA.
11 Vishnevsky National Medical Research Center of Surgery, Moscow, Russia
*Corresponding Author: Sergey Suchkov, Department of cardiology, Hospital University Center Ibn Rochd, Casablanca, Morocco.
Citation: Sergey Suchkov, Lidya Kadyrova, Matt Springer, Vladimir Zemskov, Aleksandr Tyukavin, et al, (2024), Cardiac regeneration and stem cell therapy through the view of design-driven clinical applications cardiology-related practice: current knowledge and future prospects, J. Clinical Cardiology and Cardiovascular Interventions, 7(6); DOI:10.31579/2641-0419/358
Copyright: © 2024, Sergey Suchkov. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 March 2024 | Accepted: 09 May 2024 | Published: 03 June 2024
Keywords: cardiac regeneration; cardiac stem cells; pluripotent stem cells; cardiac SCs; personalized and precision medicine (PPM)
Cardiovascular disease is the leading cause of death, with 80% of cases occurring in developing countries. Innovative therapies are required to reduce mortality and limit or abolish the necessity for cardiac transplantation. Over the last decade, stem cells have been a promise for the cure of several diseases not only due to their plasticity but also to their capacity to act in a paracrine manner and influence the affected tissue. Human SC-based therapy derivatives are extremely attractive for therapeutic development because they have direct pharmacologic utility in clinical applications, unlike any other adult cells. Moreover, stem cell-derived paracrine factors have been shown to suppress inflammation and apoptosis, stimulate angiogenesis, and amplify the proliferation and differentiation of resident cardiac stem cells (CSCs). And SC therapies are thus viable alternatives to conventional treatments with substantial therapeutic potential; market opportunities are huge, as multiple product candidates are expected to be approved over the coming decade
The ultimate goal for regenerative medicine is to channel multipotent human cells with high proliferative capacity into pre-defined scenarios and specified differentiation programs within the human body. Current therapies do not address the underlying pathophysiology of this disease, namely, the progressive loss of functional cardiomyocytes. The notion of repairing or regenerating lost myocardium via cell-based therapies remains highly appealing.
The recent identification of adult stem cells, including both cardiac stem/progenitor cells, bone marrow stem cells and others (Figure. 1)
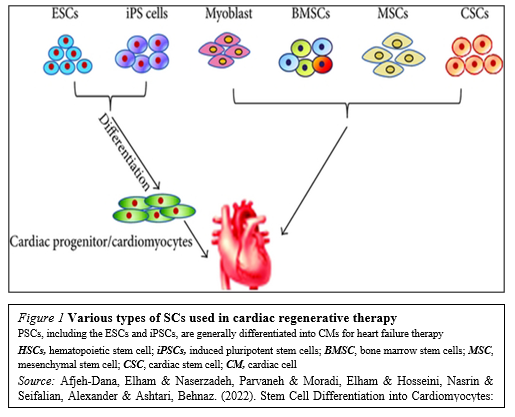
Has triggered an explosive interest in using these cells for physiologically relevant cardiomyogenesis.Unfortunately, the efficacy of cell-based therapies is somewhat limited by their poor long-term viability, homing, and engraftment to the myocardium. In response, a range of novel SC-based technologies are in development to provide additional cellular modalities, bringing CTs a step closer to the clinic. Enthusiasm for cardiac regeneration via cell therapy has further been fueled by the many encouraging reports in both animals and human studies. Further intensive research in basic science, biodesign-driven translational applications and clinical arenas are needed to make this next great frontier in cardiovascular regenerative medicine a reality.
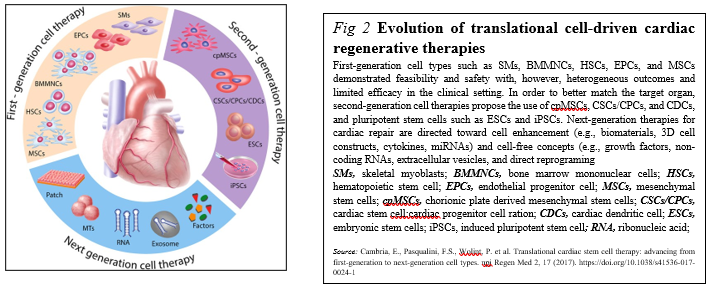
Meanwhile, stem cell (SC)-based therapy has been considered as a promising option in the treatment of ischemic heart disease (Figure. 2).
Originally, SC transplantation has emerged as a promising therapeutic strategy for acute and chronic ischemic cardiomyopathy. Regarding the current status of SC therapies for patients with myocardial infarction is critically being discussed now, describing:
(i) the current status of clinical trials of human pluripotent SCs (hPSCs) compared with clinical trials of human adult or fetal stem cells;
(ii) the gap between fundamental research and translational application of human SCs;
(iii) the use of biomaterials in clinical and pre-clinical studies of SCs; and
(iv) trends in design-driven bioengineering to promote SC therapies for patients with myocardial infarction [1,2].
Skeletal myoblasts (SMs): the pioneering steps Due to the outcome results and findings summarized, initial studies were encouraging, with SMs participating at heart muscle formation, and then were rapidly translated into the clinics with Phase I trials. However, because of the increased risk of ventricular arrhythmias potentially due to missing junctional proteins, the trials were stopped. The risk of ventricular arrhythmias is relevant now that pluripotent cell-derived cardiomyocytes aim at re-attempting heart remuscularization [3].
Bone marrow (BM)-derived cells in trials Differentiation of BM mononuclear cells (BMMNCs) into cardiomyocytes was observed but was criticized later [4].
Regarding HSCs, the researchers found no evidence of myocardial differentiation of CD34+ HSCs in preclinical models [5]. The clinical trials did not find significant beneficial effects of cell therapy [6,7].
Mesenchymal stem cells (MSCs) in trials MSCs fulfill many of the criteria for an ideal adult SC for regenerative therapy for a variety of conditions. Derived from the stromal fraction of bone marrow, MSCs can be readily isolated and identified on the basis of growth and expansion on plastic surfaces. MSCs are easily grown and expanded having multi-lineage potential, and appearing to exhibit immunological tolerance.
MSCs have repeatedly been suggested as an immunoprivileged and therefore valuable clinical cell source for cardiac repair. MSCs are multipotent stromal cells that are mainly characterized by their adherence properties, a distinct surface marker profile composed of specific markers, paracrine signaling, and the ability to differentiate into the adipogenic, chondrogenic and osteogenic lineage.
A subset of MSCs can also differentiate into cardiomyocytes under specific conditions in vitro, and thus due to the preclinical trials, adipose tissue-derived and BM-derived MSCs represent an auspicious cell source with therapeutic potential for cardiac repair, and were promising in numerous preclinical trials [8,9]. Instead of the latter, approaches using MSCs in clinical trials, are studied with promising results, but their efficacy needs to be further validated [10-12].
Second-generation therapies were aiming at orienting non-resident SCs, such as MSCs and PSCs (pluripotent stem cells), toward cardiac differentiation. Only few studies compared first-generation and second-generation cell types, which found that cardiac-committed cells displayed an improved therapeutic effect as assessed by improved engraftment, cardiac function, angiogenesis, and scar size [13-15]
Due to their enormous expansion rate and immunomodulatory properties, MSCs are considered as a potential candidate for both autologous and allogeneic SC-driven therapy with preventive, prophylactic and rehabilitative effects.
Cardiopoietic MSCs (cpMSCs) in trials The use of cpMSCs in preclinical trials with chronic ischemic disorders has shown therapeutic benefit, but the latter needs to be validated in long-term studies [16,17].
To date, clinical success of cardiac cell-therapies (including cpMSCs-driven one) remains limited. To enhance the cardio-reparative properties of SCs, the concept of lineage-specification through cardiopoietic-guidance has been recently suggested. However, so far, only results from preclinical studies and from a clinical pilot-trial in chronic heart-failure are available, while systematic evidence of its therapeutic-efficacy is still lacking [18].
Cardiac stem/progenitor cells (CSCs/CPCs) for the trials, being multipotent, clonogenic, and expressing SC markers, are usually derived directly from biopsies of the target organ, and therefore ensure a perfect match and can inhibit cardiomyocytes apoptosis [19]. Due to the preclinical studies, c-kit+ CSCs/CPCs could differentiate into cardiomyocytes, suggesting that this phenomenon occurs at a purported functionally insignificant rate [20-22].
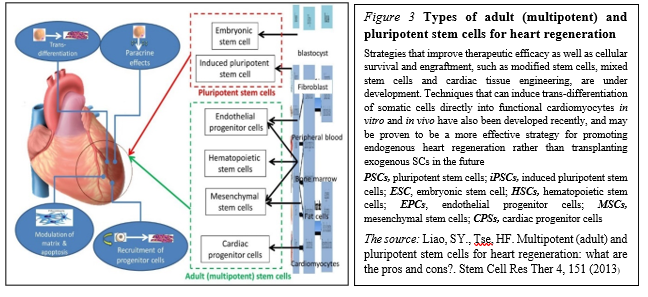
Pluripotent SCs (PSCs) in trials PSCs, including embryonic stem cells (ESCs) and induced pluripotent stem cells (iPSCs), constitute another source for guided cardiac differentiation (Figure. 3)
The most primitive of all SC populations are the ESCs that develop as the inner cell mass at day 5 after fertilization in the human blastocyst. When isolated and transferred to appropriate culture media, ESCs can undergo an undetermined number of cell doublings while retaining the capacity to differentiate into specific cell types, including cardiomyocytes.
Common teaching suggests that SCs emerging during late embryonic and fetal development are restricted to the production of tissue-specific cell types. And although SCs continue to self-renew in adult life, their ability to differentiate is limited to the tissue in which they reside, retaining a high degree of developmental plasticity. The latter would open a way to enter a revolutionary period in SC biology and regenerative medicine.
Meanwhile, human PSCs (hPSCs) are abundant sources of cardiomyocytes for cell replacement therapy and other applications such as disease modeling, drug discovery and cardiotoxicity screening [23]. And hPSC-derived cardiomyocytes have thus attracted attention as an unlimited source of cells for cardiac therapies to attract the strategy for cardiomyocyte production via the biphasic, involving hPSC expansion to generate adequate cell numbers followed by differentiation to cardiomyocytes for specific applications [24].
Preclinical studies with PSCs yielded mixed results depending on the animal model. But in most cases, human ESC-derived CPCs have been transplanted into animal models of MI, showing improved cardiac function, thus leading to clinical trials.
PSCs represent an appealing source from which to develop cell replacement therapies (Figure. 4).
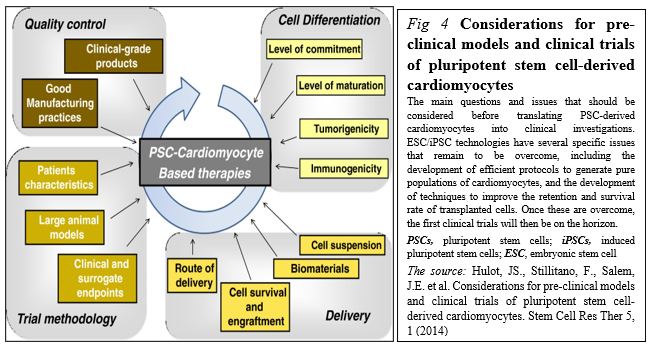
Different initiatives have been launched to promote their development toward clinical applications including stages before translating PSC-derived cardiomyocytes into clinical investigations, including the development of good manufacturing practice-level PSC lines, the development of efficient protocols to generate pure populations of cardiac myocytes, and the development of techniques to improve the retention and survival rate of transplanted cells [25].
SC-based therapies represent a possible paradigm shift for cardiac repair. However, most of the first-generation approaches displayed heterogeneous clinical outcomes regarding efficacy. Stemming from the desire to closely match the target organ, second-generation cell types were introduced and rapidly moved from bench to bedside. Unfortunately, debates remain around the benefit of SC therapy, optimal trial design parameters, and the ideal cell type [17].
Having the above-mentioned summarized and assessed, we might mention that cell (SC-driven) therapy holds potential to tackle myocardial infarction and heart failure. But the key issues such as the cell type, cell number, delivery route, timing, follow-up periods, and endpoints remain unsolved. Meanwhile, the field has rapidly evolved to address in particular the ideal cell type and does require to get the problems be surmounted to secure the full potential of cell therapy be realized in the near future to come.
1.Toward Cardiac Regeneration: Combination of PSC-Based Therapies and Design-driven Bioengineering Strategies
The potential to repair cardiac tissue by cell grafting has attracted the attention of the field, due to the scarce capacity of CMs to proliferate and replace the damaged tissue. The dispute over the existence of cardiac progenitors in the adult heart is still unsolved; on the same trail, the ability of immature cardiac progenitor cells to engraft with pre-existing CMs in vivo has not been irrefutably determined. Due to their unique capacity to produce functional CMs, a wide variety of cells have been evaluated for therapeutic
delivery, including BMCs, MSCs, and endogenous CSCs as the most promising sources for cardiac regenerative medicine application.
But despite the encouraging results from these and other in vivo studies on the potential beneficial effects of iPSC-based cell therapy for heart failure, preclinical experiments, using CMs derived from human iPSCs, have given controversial results [26]. Meanwhile, despite the fact that many different types of SCs and derivatives have been proposed as valuable candidates for regeneration of the myocardium, a general consensus on which cell type should be considered the gold standard for cell replacement therapy of the heart, remains elusive.
The problem is that the majority of preclinical studies have been conducted in 2-D culture systems, a condition that does not take into account the multiple interactions occurring in a 3-D structure, like the heart: this is among the major issues still limiting the application of cell therapy approaches into the clinics. Thus, in the last years, many productive studies have directed their efforts for the development of a 3D structure able to functionally resemble the cardiac tissue and suitable for heart transplantation.
1.1.3D culture systems as applicable to manage cardiac regeneration
In particular, the cardiac tissue is composed by contractile and non-contractile cells, that are organized as a complex 3-D structure (spheroids and organoids both referring to 3D culture systems with a specialized architecture and cell organization that typically form through self-assembling processes), which acting as tightly regulated interaction among these diverse cell types, plays a central role in the heart’s function. Thus, 3D cell cultures are emerging as a new tool for both targeted drug discovery and regenerative medicine applications, prompting and boosting the development of 3D cellular systems, as applicable to the functional features of cardiac tissue. However, those systems were found to be not ideal for developing cardiac cells for cell therapy.
The genuine true is that engineered cardiac tissue models have recently emerged as promising approaches to repair damaged cardiac tissue as well as suitable platforms for drug/toxicity testing and disease modeling (MacNeil, 2007). Meanwhile, the improvement of protocols for differentiation of PSCs toward the cardiac lineage made the production of large amounts of human CMs feasible, bursting the development of human heart surrogates for disease modeling, drug testing and autologous cell therapy applications. On this regard, embedding CMs derived from PSCs into engineered structures has been shown to positively impact cell maturation to different extents, depending on the specific characteristics of the generated 3D-constructs. In fact, use of both human iPSCs and ESCs deals with an important issue of cell maturation following cardiac induction in vitro [27]. Thus, altogether these studies strongly indicate that the above-mentioned constructs are excellent supports for maturation of CMs derived from human PSCs, since they provide a physiological-like environment and stimuli to cells. And, moreover, altogether those studies showed that cardiac engineered constructs enhance intercellular organization and crosstalk of iPSC-CMs, improving their maturation in vitro, and ameliorate cardiac performance after the transplantation in vivo, thus providing encouraging evidences for their future use to achieve cardiac regeneration in humans.
A significant number of different cell therapy strategies that employ iPSC-CMs have been proposed to restore cardiac function, ranging from injection of cells alone, to their combination with ECM-like biomaterials, and to more complicated engineered-based strategies, which aim to faithfully recreate the myocardium.
Although different types of stem cells have been proposed as potential candidates for cardiac regenerative medicine, there is no consensus about which represents the best choice. Given the complexity of cardiac tissue, which is composed by diverse cell types, human PSCs – mostly iPSCs – are certainly among the most relevant sources. In particular, CMs differentiated from iPSC may represent a realistic option for the regeneration of the injured heart (Figure. 5)

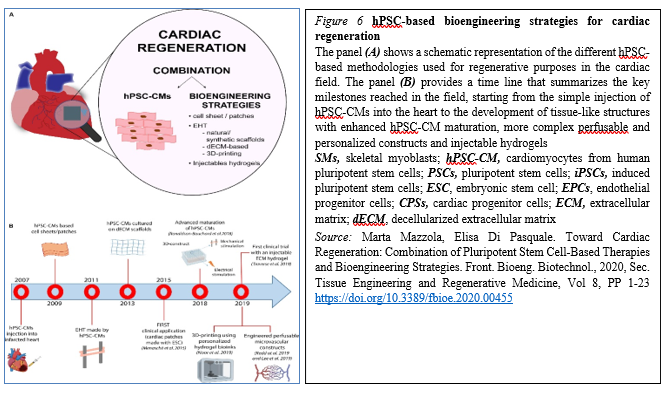
The majority of these approaches have shown – at least to some extent – success in mimicking heart cells and improving cardiac function, providing new hope for the replacement of CMs after the irreversible loss of heart tissue occurring during myocardial infarction (Figure 6).
The progress in the field made by tissue engineering technologies has been encouraging and thus opened ways to create bio-supports able to incorporate the cells needed for the regeneration of cardiac tissue. However, significant improvements are still mandatory before we could consider their routine use in the clinical field for treatment of patients suffering from myocardial diseases. These improvements mainly regard scaffold production, the interactions between cells and the ECM and vascular integration with the host, hopefully opening new doors for cardiac regeneration therapy via tissue engineering strategies. However, despite the promising results obtained by preclinical research, the approach is still rather immature for its clinical translation and further investigations are needed to develop effective and more efficient strategies to achieve cardiac regeneration in vivo.
1.1.Engineered cardiac tissue constructs to be translated into clinical applications
No comments, but design-driven tissue engineering strategies are probably a more suitable option. And given the limited regenerative capacity of the heart, the design-driven bio-engineered scaffolds and tissue engineering approaches are thus ideal for cardiovascular regenerative medicine applications. The main goal is to create a cardiac graft which can be implanted and restore the functionality of the myocardium without major side effects. To this aim, tissue engineering intends to recreate the microenvironment of the cardiac tissue, in terms of cell composition, stiffness, geometry, physical and electrical stimuli and, extracellular matrix, and in order to generate constructs with an actual translational value, keeping in mind the native characteristics of the cardiac tissue [28] .And although SC therapy is a promising treatment for myocardial infarction, the minimal functional improvements observed clinically limit its widespread application. Where a need exists to maximize the therapeutic potential of those SCs by first understanding what factors within the infarct microenvironment affect their ability to regenerate the necrotic tissue, and to define a novel mechanism by which the extracellular environment of the infarction regulates the therapeutic potential of MSCs.
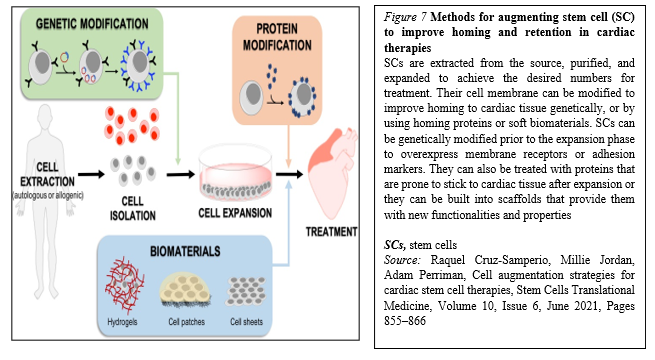
Moreover, within the last years, many biomaterials have emerged as good candidates for cardiac tissue engineering to fill the existing gap for their application to cardiac regeneration and treatment of myocardial infarction, and to increase cell retention, improving cell survival and coupling with the host. In general, cell homing and adhesion to cardiac tissue can occur via specific receptor-mediated interactions with the extracellular matrix (ECM) proteins, or can be initiated via physical/chemical adhesion to cardiac cells via hydrophobic and electrostatic interactions. It is widely accepted that SCs target inflammation and injury sites, including infarcted myocardium. Accordingly, many SC membrane reengineering approaches aim to promote these endogenous processes, whilst describing the development of new targeting strategies to improve homing efficiency (Figure. 7).
The fast-growing development of new technologies to reengineer the membrane of SCs or provide a supporting biocompatible matrix may alleviate these limitations. It is clear that genetic approaches are extremely exciting, as they can be implemented through reliable protocols that are easy to track in the preclinical phase, and have a low risk of triggering unwanted immune responses.
With respect to the developments within the biomaterial scaffold space, although they offer an effective solution to myocardium cell retention and cell number, the transplant process is generally more invasive, and challenges with effective electromechanical integration still remain. Meanwhile, the scaffolds could be modified or implemented in combination with molecules that activate the recruited cells (e.g., statins) and amplify their therapeutic potential. In conclusion, it is likely that no single approach to SC membrane reengineering will provide the “magic bullet” for cardiac cell therapies, and that the next generation of therapies will likely utilize combinations of these technologies to fully harness the therapeutic potential of transplanted SCs.
However, regardless of the employed strategy, generation of tissue-like engineered structures suitable for regenerative cardiology applications needs further considerations, specifically in relation to some aspects that may be critical for their efficacy and potential undesired effects in vivo.
2.Cardiac SCs (CSCs) as promising cell types for cardiac regeneration
Myocardial infarction results in an irreversible loss of cardiomyocytes due to aging or pathophysiological conditions, which is generally considered irreversible, and can lead to lethal conditions with subsequent adverse remodeling and heart failure. But human PSCs, including ESCs and iPSCs, can self-renew while maintaining their pluripotency to differentiate into all cell types, including cardiomyocytes. So, identifying new sources for cardiomyocytes and promoting their formation represents a goal of cardiac biology and regenerative medicine.
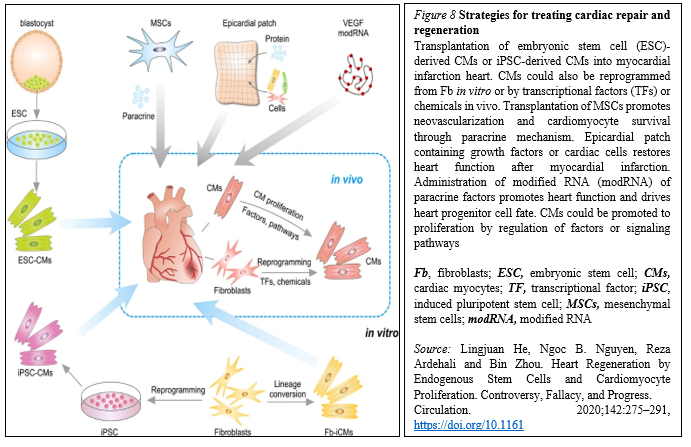
Meanwhile, because of the lack of strong evidence supporting the existence of resident CSCs, efforts are focused on how to mobilize and promote those few cardiomyocytes that have potential to proliferate in mammalian hearts. Whereas endogenous cardiomyocytes can proliferate at a low frequency, methods that promote cardiomyocyte proliferation may be a vital research field in the future. The aforementioned pathways could be manipulated, optimized, and synergized to achieve better functional improvement after cardiac injury. In addition to inducing cardiomyocyte proliferation, other alternative approaches could be considered (Figure. 8).
In situ reprogramming of fibroblasts to cardiomyocytes by overexpression of specific transcriptional factors represents a promising direction for future study [29].
Recent studies have also suggested that small molecules can induce reprogramming of fibroblasts to cardiomyocytes in vivo, which offers a dual pharmaceutical approach to regenerate cardiomyocytes and reduce scar formation [30].
Human ESCs or iPSCs-derived cardiac progenitors and cardiomyocytes have been successfully transplanted and confirmed the survival of transplanted cells within the host myocardium and an improvement in cardiac function after injury. Furthermore, dual SC therapy, such as human iPSC-derived cardiomyocytes and MSCs, or human ESC-derived epicardium and cardiomyocytes, synergistically improves cardiac function and augments vascularization in the injured myocardium. Moreover, recent advances in engineered epicardial patch containing multiple cardiac cell types are improved heart function and neovascularization after myocardial infarction [31-33].
In this context, CSCs are considered to be very promising cell types for cardiac regeneration. And within the past decade, among cardiac myocytes many types of putative CSCs have been reported to regenerate the injured myocardium by differentiating into new cardiomyocytes. Some of these CSCs have been translated from bench to bed with reported therapeutic effectiveness. However, recent basic research studies on stem cell tracing have begun to question their fundamental biology and mechanisms of action, raising serious concerns over the myogenic potential of CSCs [34]
In partocular, c-Kit+ CSCs represent a promising candidate for cardiac-specific SC lineages, which is likely heterogenous in nature [35]. The 1-year follow-up results from the SCIPIO trial support that intracoronary infusion of one million autologous c-Kit+ CSCs in patients with heart failure of ischemic etiology undergoing coronary artery bypass grafting is safe and feasible and may promote significant improvements in global heart function, decrease scar size, and induce regeneration of viable myocardium.
As you might see, resident CSCs are self-renewing and can give rise to cardiomyocytes. Their multipotentiality allows them to differentiate along the three main cardiac lineages: myocytes, endothelial cells, and smooth muscle cells. After their injection in the ischemic heart, the formation of the above-mentioned cell types contributes to the regeneration of myocardium and the improvement of its contractility.
But the approaches securing cardiac regeneration in post-infarction period are not available to be practiced. And the key problem is the identity of cells be born to generate functionally active cardiac myocytes replenishing those being lost during ischemia.
Previous research made by several groups has identified an extensive population of CSCs in the adult heart. Through the view of the latter, there are four ongoing clinical studies to test the benefits of autologous CSCs:
Meanwhile, with identification of resident CSCs (rCSCs), it has been supposed that the latter may be a crucial source to initiate and prompt myocardial self-renewal and regeneration. But along with the latter, endogenous cardiomyogenic SCs (CMSCs) might be better choice for cardiac repair. Ideally, those cells should be directly stimulated in situ, avoiding extraction, purification, culture and reinjection. It is therefore of uttermost importance to understand the identity and function of the cells that constitute the natural environment of cardiac progenitors and support their quiescence, self-renewal and activation. Additionally, further studies are needed to develop a deeper understanding about the properties of pericytes, as these cells have the potential to migrate to different tissues away from their perivascular location and play an active role in the activation of cardiac repair after ischaemia. This would involve a modern interpretation of the pericyte’s role as a cell type involved in reducing the threshold for the activation of an angiogenic program in cardiac repair [38].
CSC therapy holds great potential to prompt myocardial regeneration in patients with ischemic heart disease. The selection of the most suitable cell type is pivotal for its successful application. Various cell types, including crude bone marrow mononuclear cells, skeletal myoblast, and hematopoietic and endothelial progenitors, have already advanced into the clinical arena based on promising results from different experimental and preclinical studies. However, most of these so-called first-generation cell types have failed to fully emulate the promising preclinical data in clinical trials, resulting in heterogeneous outcomes and a critical lack of translation. Therefore, different next-generation cell types are currently under investigation for the treatment of the diseased myocardium [39].
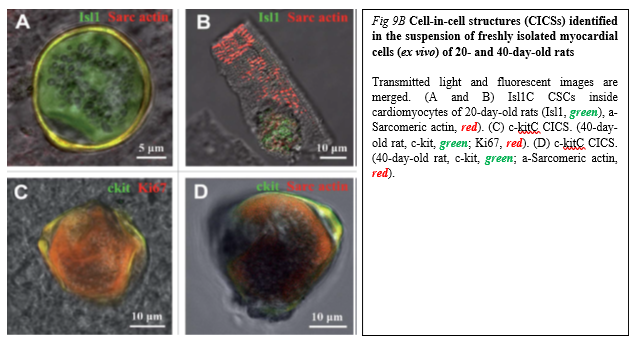
Drug (including SC-driven) development continues to move in the direction of Personalized and Precision Medicine (PPM), - where ideally the most effective therapy or treatment is determined by the genetic makeup of the patient and thus by a spectrum of biomarkers to be targeted by the therapeutics (including those being based on SCs). Regarding PPM-based cardiology practice and the innovations made in the field of SC-driven technologies, the focus in the last years has been moved towards a concept of the new wave of cardiac myocyte (CM) formation via a scenario of dedifferentiation and proliferation of mature CMs. The observation that CSCs can be developed inside a pool of immature cardiac cells by formation of “cell-in-cell structures” (CICSs) has enabled us to conclude that CICSs being encapsulated are implicated into mammalian cardiac myogenesis over the entire lifespan (Figure. 9A,B).

It had been demonstrated before that new CMs are generated through formation of CSC-derived transitory amplifying cells (TACs) either in the CM colonies or in a process of intracellular development of CICSs being encapsulated.
The analysis of adult rat cardiac cell suspension 1-5, 10, and 14 days after permanent coronary occlusion and ischemia/reperfusion has gifted a researcher a unique phenomenon of TAC release from mature CMs with clear sarcomeric structure. In this case a development of the intracellular CSC occurs within the vacuole pre-formed by CSC-driven sarcolemma-induced invagination. The comparison of TACs exiting the CICS with capsule with TACs just released from non-encapsulated CICS showed that non-encapsulated CICS-derived TACs are characterized by increased expression of cardiac markers and decreased expression of stemness-related markers.
Earlier on syngeneic animals using the label - GFP was shown that a local laser apoptotic effect on tissues causes an intensive transition of mesenchymal BMSCs from the bloodstream to the zone of programmed cell death (Figure. 10).
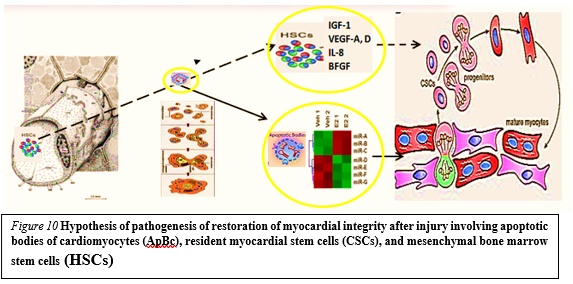
Apoptotic bodies (ApB) of cardiomyocytes combine the functions of CSC and HSCs in the areas of myocardial regeneration. Signaling molecules are located on the surface of ApB, which mediate the homing and chemotaxis of HSCs to the area of the damaged myocardium. HSCs provides targeted delivery of growth factors and cytokines required to maintain CSC proliferation.
ApB contains a complex of molecules, carriers of "epigenomic memory" about the tissue belonging of a dead cell. It is likely that simultaneously with the triggering of the effector link of apoptosis, which ends with the formation of ApB, RNA is expressed, the new profile of which is the “code” of the tissue belonging to the dead cell. When ApB enters the CSC via endocytosis, a specific set of long and short non-coding RNAs express genes that determine the direction of differentiation of resident myocardial stem cells. It can be assumed that this hypothesis is true not only for the heart, but also for other organs and tissues [40].
Those data for the first time suggest that the development of CSCs inside the encapsulated CICSs is important for cardiac self-renewal and maintenance of CSC-based pool. At the same time, the development of CSCs inside a population of mature CMs is resulting in the formation of pre-cardiac myocytes, which are able to substitute for irreversibly injured CMs, representing the major mechanism of myocardial regeneration. And that, in turn, would open up a green light to secure the targeted management of regenerative cardiac myogenesis. So, the formation of new cardiomyocytes within the injured myocardium has not been conclusively demonstrated.
Meanwhile, SC therapies are viable alternatives to conventional treatments with substantial therapeutic potential and market opportunities. And the lessons learned from our studies would yield fundamental biological insights in the repair of ischemic and other myocardial diseases whilst securing the therapeutic resources with the unique future.
To stress the above-mentioned, Biodesign-inspired and biotech-driven translational research & applications are keeping success in the field elusive in terms of return on investment and in terms of attractiveness to investors within and outside of biopharma and SC-related market as well. The SC market itself is predicted to grow to around $12.1 billion by 2024, whilst the development of the SC therapy into further applications has not yet become common practice, and the true potential of regenerative medicine has yet to be demonstrated fully. For instance, the allogeneic or ‘off-the-shelf’ business model for SC-based therapies is far more akin to current biopharmaceuticals, where the product maintains long-term stability. Meanwhile the global SC therapy market for cardiovascular disorders is likely to grow to $3.3 billion by 2030, driven by the rising incidence of those disorders.
However, the translation of SC therapy for heart diseases from bench to bed is still hampered by several limitations, covering some barriers dictated by the clinical application of SC-based therapies, the investigation of mechanisms behind SC based cardiac regeneration and also, what bioengineers can do and have been doing on the translational stage of SC therapies for heart repair. In this context, the biotech company CardioCell announced effective results in the application of SCs for the treatment of chronic heart failure indications at the European Society of Cardiology Congress, presenting the outcome of preclinical and clinical trials to study the effects of intravenous ischemic tolerance to MSCs in the treatment of chronic heart failure [41].
During the same year, at the annual meeting of the Society for Cardiovascular Angiography and Interventions (SCAI), a number of experts announced promising results for the RENEW trial and the ATHENA (Autologous adipose-derived regenerative cells for refractory chronic myocardial ischemia with left ventricular dysfunction) trial. Although the results of these trials did not sufficiently show significant efficiency due to the early termination and limited sample size, they could still be promising development demonstrating the potential for viable SC-based heart therapies.
Meanwhile, design-driven engineering methods (Figure. 11)
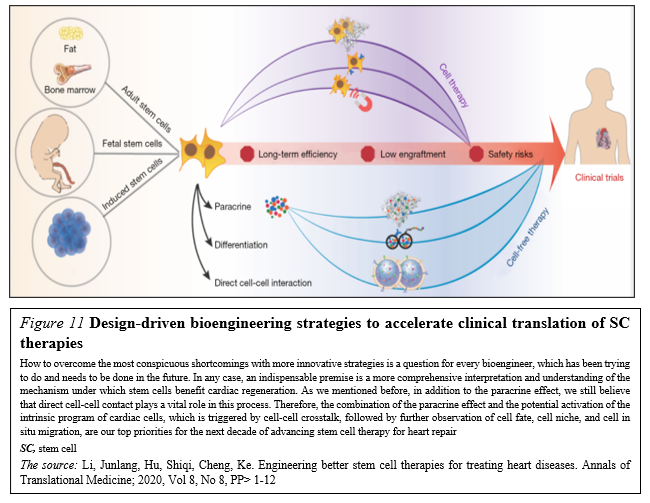
that aim to realize the multifunctionalization of SC therapies have been thriving in the past five years. With the collaboration of physicians, chemists, biodesigners and bioengineers are able to develop SC-based therapies that combine SCs, or their byproducts, with biomaterials in order to enhance therapeutic efficiency and to secure the effective delivery and biosafety [42].
So, SC research and translational applications have made significant progress in the field of cardiovascular regenerative medicine over the past few decades. However, there is still a long way to go before SC therapy can be safely and effectively applied in clinical practice. But moving forward, we must better characterize SC-based therapy and clinical trials, facilitating decision making across the sector. More basic science investigation is required to elucidate the specific mechanism(s) by which SC promote cardiac regeneration and/or repair, and how cells can be optimally delivered and engineered. As our understanding of SC therapy increases, it becomes more likely that clinical trials can produce truly meaningful results with implications for clinical practice.
Based on the new mechanisms and unique phenomenon, we are developing improvement strategies to boost the potency of SC repair and to generate the “next generation” of SC-based and regulatory biomolecules-based (bimodal) therapeutics. Moreover, our strategies should aim at more personalized SC therapies in which individual disease parameters influence the selection of optimal cell type, dosage and delivery approach. And encouraging pre-clinical and clinical studies as one and solid entity reporting significant SC-mediated cardiac regeneration would rapidly pave the way for clinical translation. So, a desire to discover innovative SC-based technologies of the next-step generation would encourage governments and companies to focus directly on regenerative medicine as a future potential economy and social insurance booster.
Thus, prospective research should focus on the development of specific responder scores and the identification of prognostic SC- and cardiac damage-related biomarkers to identify patient cohorts who benefit most from distinct SC treatments. Thereby, a higher standardization of study designs and the establishment of a global open-access database for the registration and publication of pre-clinical and clinical trials would greatly improve the comparability and access of obtained data.
In reality, the global (worldwide) SC therapy market is still in an early stage. And the developing translational pipelines for rising applications will build the competition among merchants amid the conjecture time frame.
Consequently, the focus of research in the field has since shifted to SC-derived paracrine factors, including cytokines, growth factors, mRNA, and miRNA. Notably, both mRNA and miRNA can enter into the extracellular space either in soluble form or packed into membrane vesicles. SC-derived paracrine factors have been shown to suppress inflammation and apoptosis, stimulate angiogenesis, and amplify the proliferation and differentiation of resident cardiac SCs (CSCs). Such features have led to exosomes being considered as potential drug candidates affording myocardial regeneration.
The search for chemical signals capable of stimulating cardiomyogenesis is ongoing despite continuous debates regarding the ability of mature cardiac myocytes to divide or dedifferentiate, trans-differentiation of other cells into cardiac myocytes, and the ability of CSCs to differentiate into cardiac myocytes. Future research is aimed at identifying novel cell candidates capable of differentiating into cardiac myocytes. The observation that CSCs can undergo intracellular development with the formation of “cell-in-cell structure” and subsequent release of transitory amplifying cells with the capacity to differentiate into cardiac myocytes may provide clues for stimulating regenerative cardiomyogenesis.
Indeed, human SC-based therapy derivatives are extremely attractive for therapeutic development because they have direct pharmacologic utility in clinical applications, unlike any other adult cells. The human SC as a special entity is emerging as a new type of potential therapeutic agent of cellular entity in cell-based regenerative medicine, because human SC-based therapy derivatives have the potential for human tissue and function restoration that the conventional drug of molecular entity lacks.
In this context, realizing the translational and therapeutic potential of CICSs has been hindered by some obstacles which would be surmounted and brought SC-based therapy of the future towards clinical applications, including establishing defined culture systems for de novo derivation and maintenance of clinical-grade progenitor cells and lineage-specific differentiation of the latter by siRNA-driven modulation. Such milestone advances and medical innovations in CICSs research allow generation of a large supply of clinical-grade cardiac progenitor-based therapy derivatives targeting for cardiac problems, bringing cell-based regenerative medicine to a turning point. We expect that advanced modalities that integrate cellular, bioengineering, and information (IT) technologies via clinical studies and translational applications as new consolidated entities will enhance the efficacy of cardiac cell therapy and further contribute to cardiac regenerative medicine.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
