
Review Article | DOI: https://doi.org/10.31579/2693-2156/002
*Director of Clinical Research The Heart and Vascular Institute 7205 Wolf Rvr. Blvd. Germantown, TN, USA
*Corresponding Author: Gary L. Murray, Director of Clinical Research The Heart and Vascular Institute 7205 Wolf Rvr. Blvd. Germantown, TN, USA.
Citation: Gary L. Murray, (2020) Cardiac Perioperative MACE: Could Ranolazine Safely Reduce it ≥ 35%?. J Thoracic Disease and Cardiothoracic Surgery, 1(1); DOI: 10.31579/2693-2156/002
Copyright: © 2020 Gary L. Murray, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 31 March 2020 | Accepted: 08 April 2020 | Published: 15 April 2020
Keywords: ranolazine; perioperative; MACE; cardiac surgery
The Society of Thoracic Surgery Score and Euro II Score are tools for estimating major adverse cardiac events (MACE [death {or morbidity}, renal failure, stroke, prolonged ventilation, CSW infection, reoperation, prolonged admission]) after cardiac surgery.
Short Title: Ranolazine and Cardiac Perioperaive MACE
The Society of Thoracic Surgery Score and Euro II Score are tools for estimating major adverse cardiac events (MACE [death {or morbidity}, renal failure, stroke, prolonged ventilation, CSW infection, reoperation, prolonged admission]) after cardiac surgery. Although deaths average approximately 3%, predicted mortality can exceed 20% [1]. Hyperlactatemia occurs in 1.3%, most commonly due to acute congestive heart failure (CHF) [2].Chronic CHF patients suffer Vasoplegia in 29% [3]. Troponin elevations are frequent, although an AMI diagnosis incidence is 3% (up to 12%), most commonly after surgery involving the mitral valve or cardiac arrest [4-7].Post- operative ventricular arrhythmias (POVA) are present in 1.7% of patients, more commonly in the elderly, those with chronic CHF, after emergency surgery, or when left ventricular mass index is > 188m/m2 [8,9].
We are as poor in mitigating perioperative MACE as we are as good at predicting it. Amiodarone and chronic beta blockade help some [4,10], but we need more. I propose ranolazine may be our safe pharmacologic salvation, as a result of my 14 years’ experience with its use in coronary disease, congestive heart failure, and ventricular arrhythmia (also atrial fibrillation). I will briefly detail my published studies done in non-surgical patients below; I have no reason to suspect that any of ranolazine’s profound benefits (37-40% MACE reduction) would not occur perioperatively.
Ranolazine has 2 main mechanisms of action (MOC) [11-15]:
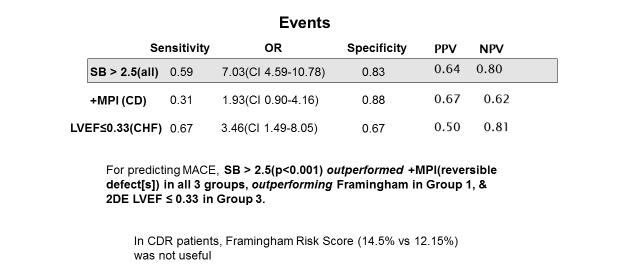
1. Strong use-dependent inhibition of neuronal sodium channel 1.7 (Nav1.7 ) in its open state via the local anesthetic receptor. This reduces high Sympathovagal Balance (SB) and can also correct Cardiac Autonomic Neuropathy (CAN = critically low Parasympathetic tone [RFa < 0 r=0.0048, p=0.02140;> 2.5, 55% of patients suffered MACE (cardiac death, acute coronary syndromes, elective revascularization, ventricular tachycardia/fibrillation, CHF admission) (r=0.0117, p=0.0108). SB > 2.5 increased MACE 7- fold (11) in 483 patients with risk factors or established CAD or CHF, mean f/u 4.92 yrs (Table 1).
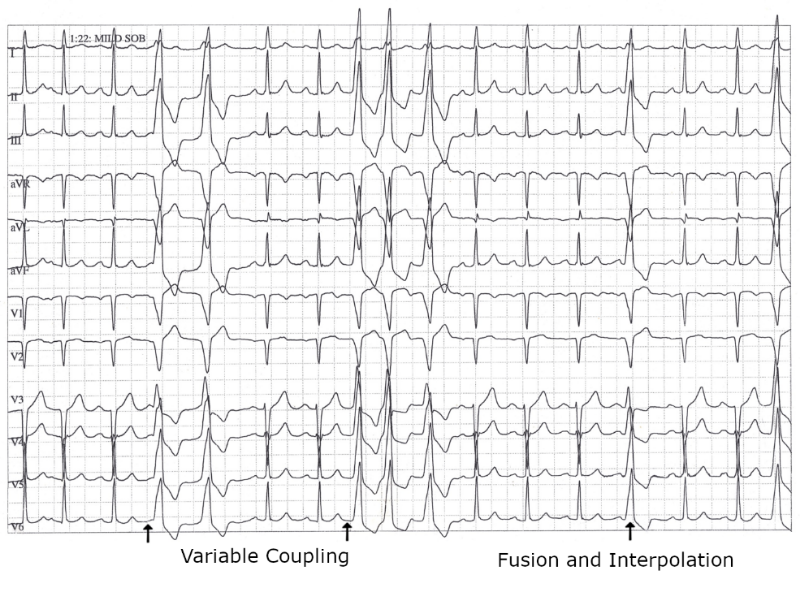
2. Inhibition of the cardiac Nav1.5 late inward sodium current( INa ) by attaching to Nav1.5 ‘s amino acid F 1760. Nav1.5 ‘s opening 1 msec (the early INa ) results in the upstroke of the QRS complex and systole. Any stress, including surgery, can result in faulty gating of the sodium channel, causing a marked increase of the late INa . The resulting high myocellular Na+ is exchanged for Ca++ via the Na+/Ca++ exchanger (NCX).Therefore, both Na+ and Ca++ are elevated, resulting in increased diastolic dysfunction, increased triggered ventricular arrhythmias due to early and delayed afterdepolarizations [15] (EAD/DAD, Figure 1, Table 2), diastolic compression of the coronary microvasculature yielding myocardial ischemia, and depression of left ventricular ejection fraction (LVEF).
The Ca++ overload results in mitochondrial dysfunction, reduced ATP, and increased oxidative stress-all of which occur during the reperfusion injury of cardiac surgery (16), depressing LVEF. Ranolazine mitigates this [16,17].
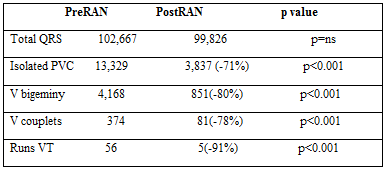
*95% (56/59) of patients had their ventricular ectopy reduced by ranolazine. PVC = premature ventricular contractions; RAN = ranolazine; V = ventricular; VT= ventricular tachycardi.
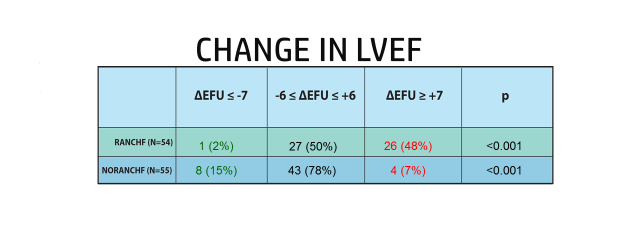
In our studies, when ranolazine was added to guideline therapy in 81 CHF patients, over 1-2 yr. mean f/u in these 2 studies, high SB corrected in 83% of patients (p=0.033), and CAN improved in 67% (12), LVEF increased in 70% of patients an average of 11 ejection fraction units(EFUs) (p<0>
In our CAD study [14], mean f/u 6 yrs., ranolazine reduced MACE(acute coronary syndromes, elective revascularization, cardiac death) by 37%(p=0.0105). In our triggered Ventricular arrhythmia study (15),(Figure 1, Table 2), 95% of patients responded to ranolazine.
Ranolazine and Cardiac Surgery Mace
In light of these studies, ranolazine should reduce perioperative CHF, ventricular (and atrial) arrhythmias, and ischemia. It might reduce the vasoplastic syndrome as well. In this syndrome, there is a dramatic increase in sympathetic (S) tone. The resulting high beta 2 stimulation of the vasculator contributes to the refractory vasodilatation characteristic of this syndrome [3]. Ranolazine should reduce S, allowing vessels to be more responsive to vasopressor therapy.
Is there a downside to ranolazine? Not that I can fathom. In the 14 yrs. since its launch, I know of not a single death attributed to it. Its most frequent side effects (6% of patients) are headache, dizziness w/o BP change, nausea, and constipation. There may be a tiny, clinically insignificant creatinine increase, and Hgb A1C decreases by 0.6% It steady states by 72hr (precisely when perioperative MACE peaks), is metabolized by CYP3A (so cut statin dose ½),and interacts with P-gp (reduce digoxin dose ½) and OCT2(limit metformin to 1700 mg/d). Do not use in patients with stage 4 or 5 chronic renal disease. The other absolute contraindication is ranolazine allergy. It can be used with any antiarrhythmic. Torsades de pointes requires [1] prolongation of the QT interval (usually to > 500msec); [2] afterdepolarizations; and [3] transmural dispersion of repolarization. Ranolazine only prolongs the QT 6msec, reduces afterdepolarizations, and does not cause dispersion of repolarization [13,15].
Based upon my publications, ranolazine should reduce perioperative complications:
should be taking ranolazine regardless of needed surgery, not just because of it. Start 500mg b.i.d. p.o., attempting to increase to 1000mg b.i.d. p.o. after 3d, at least 1-4wks.preoperatively. If surgery is an emergency or urgent, start 1000mg b.i.d. as soon as the patient can start it.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
