
Short Communication | DOI: https://doi.org/10.31579/2693-7247/081
1School of Pharmaceutical Sciences, Jaipur National University, Jagatpura, Jaipur, Rajasthan 302017, India.
2Quantum School of Health Sciences, Department of Pharmacy, Quantum University, Roorkee, Uttarakhand, 247662, India.
*Corresponding Author: Sadique Hussain, School of Pharmaceutical Sciences, Jaipur National University, Jagatpura, Jaipur, Rajasthan, India.
Citation: Sadique Hussain, Swati Tyagi, (2022). Cardiac Management in Covid-19 Patients. Journal of Pharmaceutics and Pharmacology Research. 5(5). DOI: 10.31579/2693-7247/081
Copyright: © 2022 Sadique Hussain. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 March 2022 | Accepted: 28 March 2022 | Published: 22 April 2022
Keywords: cardiac management; cardiac patient; covid-19
Coronavirus disease 2019 (COVID-19) was initially identified in late December 2019 in Wuhan, China. COVID-19 has spreaded swiftly over the planet, becoming a global pandemic affecting over 200 nations and territories, having an extraordinary impact not only on public health but also on social and economic activity.
Coronavirus disease 2019 (COVID-19) was initially identified in late December 2019 in Wuhan, China. COVID-19 has spreaded swiftly over the planet, becoming a global pandemic affecting over 200 nations and territories, having an extraordinary impact not only on public health but also on social and economic activity [1-3]. The exponential surge in the number of COVID-19 patients over the last 6 months has overburdened health-care systems in several nations throughout the world [4]. With the rapid increase in confirmed cases, the cardiovascular diseases (CVDs) induced by SARS-CoV-2 have generated considerable concern. A study of 138 hospitalized patients with COVID-19 showed that 7.2% had an acute myocardial injury. Huang et al. reported that 12% of COVID-19 patients were diagnosed as having an acute myocardial injury. COVID-19 patients with underlying coronary artery disease (CAD) who develop myocardial injury (MI) were found to have poorer in-hospital outcomes [5,6].
Patients with COVID-19 who have cardiac difficulties are at a greater risk of morbidity and death. They may have the following cardiac complications: worsening of a prior cardiac issue, acute heart failure (AHF), acute myocarditis, acute coronary syndrome (ACS), acute stent thrombosis, venous thromboembolism, and different arrhythmias. Some individuals may arrive with ACS-related ECG abnormalities but non-significant lesions. Other people may have severe cardiomyopathy with normal coronaries (Takotsubo-like syndrome). Some individuals may experience negative effects with COVID-19 medication, such as the hydroxychloroquine-azithromycin combination, which can result in a deadly extended QT interval. These patients should be investigated as follows: CBC, ESR, CRP, D dimers, cardiac troponin, ECG (to assess ischemia, arrhythmia, and QT interval), CXR (to assess signs of cardiomegaly or pneumonia), echocardiography (to assess LV diastolic dysfunction, LVEF, valvular lesions, and pericardial effusion), coronary angiography if indicated, PCR to nasopharyngeal swabs and CT chest. Most cardiac drugs, such as antiplatelets, statins, and RAS blockers can be safely continued after the diagnosis of COVID-19 [7,8].
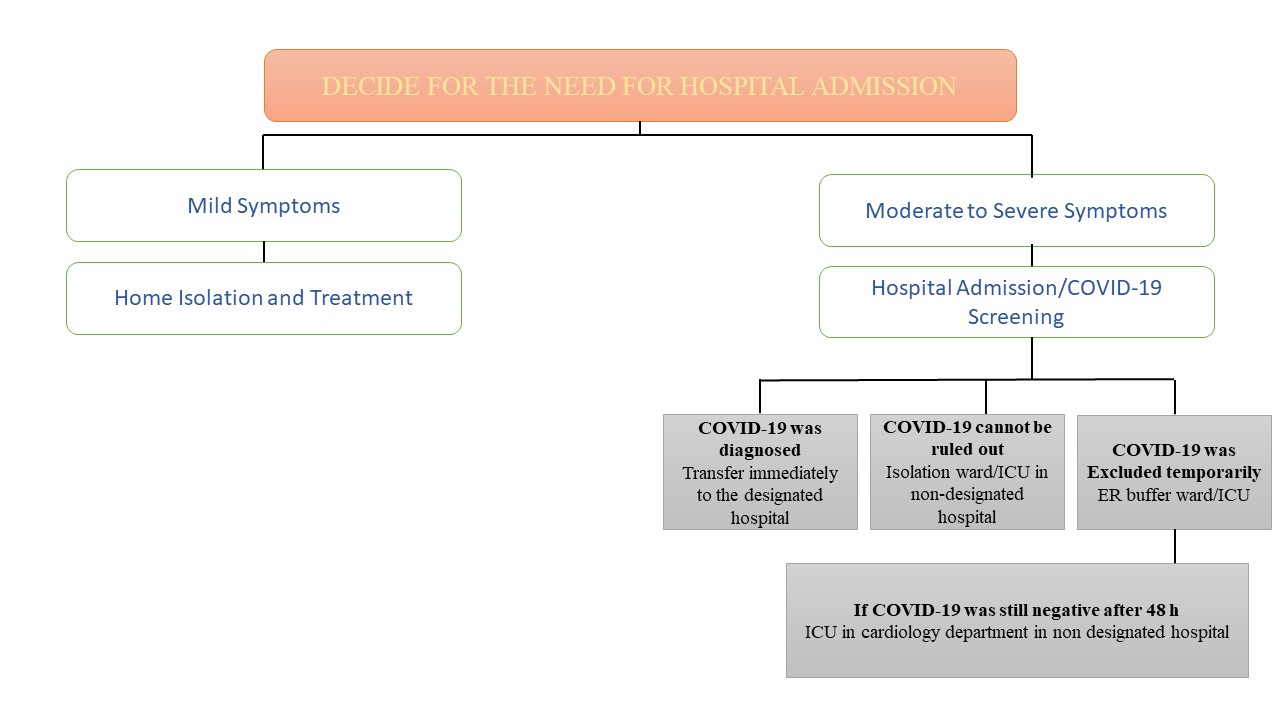
During the pandemic, hospitals should be divided into two main categories:
A. COVID-19 designated hospitals—for patients infected with the virus. These hospitals will need all specialties including cardiologists.
B. Non-COVID-19 designated hospitals—for noninfected patients with other diseases. Yet, due to the long incubation period of the virus and the presence of asymptomatic infection, the potential infection risk of medical staff in non-designated hospitals exists. Moreover, some COVID-19 patients may present with what looks like cardiac complaints and this puts cardiologists at risk of getting the infection [9].
Patients with CVDs are more likely to suffer a MI and have a poor prognosis. CV biomarkers should be regularly tested on all COVID-19 hospitalised, especially those with pre-existing CVDs. Although these individuals required very minor cardiac care, the CVDs was found to be strongly associated with death in COVID-19 individuals. Increased TnT levels may aid in the identification of high-risk individuals and may need a change in care plan. Furthermore, cardiac concerns may be concealed since individuals who diagnosed with severe respiratory problems might swiftly worsen before cardiac difficulties become evident [10].
Managing CV risk factors may thus safeguard against more chronic COVID-19 disease. To do this, innovation must be applied in novel ways. Teleconsultations are used to provide general care and cardiac support in various nations. When services are disrupted for an extended period, pragmatic methods to person monitoring are required. Certain medical gadgets and mobile applications, for example, might be used to detect arrhythmias [11].
There is a need to determine the most critical CV complication that might contribute to the development of the illness to focus medical personnel's attention on potential problems. Additionally, psychological counselling should be offered to individuals to ensure that everyone is aware of the facts of the matter and to better equip people to deal with their hospitalisation and following COVID-19 follow-up [12]. Patients with high blood pressure, diabetes, and/or obesity are a high-risk category that should be constantly watched in hopes of avoiding or cure potential consequences from SARS-CoV-2 illness. Males and individuals over the age of 60 with serious infection are of particular concern, as they have been demonstrated to have a longer duration of virus in stool, serum, and respiratory samples [13]. We presently have little information on the potential CV problems that may emerge because of CoV. So far, there has only been speculation regarding the molecular impacts on cardiomyocytes and endothelial cells, as well as a probable elevated risk of HF in the future. Nevertheless, due to the rising recognition of CVD impairment in this condition, a longer term follow up of severe COVID-19 survivor will be required to answer this issue.
The World Heart Federation Science (WHF) Committee will continue to closely monitor the evolving nature of the data on COVID-19 and its potential link with CVDs. They strive to keep updating the latest information on the clinical implications of COVID-19 outbreak on CVDs and organize webinars involving expert panellists to share experience of the front-line health workers managing COVID-19 and CVDs. Furthermore, WHF COVID-19 CVD global survey will provide key insights to inform clinical and policy practices, for a better understanding of the CVDs that increase the risk of developing severe COVID-19, and a better characterization of cardiovascular complications in hospitalized patients with COVID-19.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
