
Research Article | DOI: https://doi.org/10.31579/2641-0419/145
*Corresponding Author: Heyder Omran, GFO Kliniken Bonn, Robert-Koch-Str. 1, 53115 Bonn, Germany
Citation: Jaroslaw Heinrich, Baravan Al-Kassou, Heyder Omran., (2021) Cardiac Computed Tomography versus 3D-Transesophageal Echocardiography in Preprocedural Planning of Left Atrial Appendage Closure. J. Clinical Cardiology and Cardiovascular Interventions, 4(6); Doi:10.31579/2641-0419/145
Copyright: © 2021 Heyder Omran, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 February 2021 | Accepted: 11 March 2021 | Published: 18 March 2021
Keywords: left atrial appendage closure; imaging modalities; cardiac computed tomography; transesophageal echocardiography; 3D transesophageal echocardiography
Aim:
Preprocedural imaging of the left atrial appendage (LAA) plays a crucial role in the process of LAA closure (LAAC). This study aimed to compare the influence of preprocedural planning of the LAAC with 3D-transesophageal echocardiography (TEE) and cardiac computed tomography (CCT) versus 3D-TEE alone in patients who underwent LAAC with an Amplatzer Cardiac Plug or Amulet.
Materials and Methods:
In a retrospective study, 176 patients received a preprocedural 3D-TEE and CCT and 167 patients a 3D-TEE only. Both groups had similar patient characteristics and indications for LAAC.
Results:
There was no difference in terms of procedural success, procedure time, amount of contrast medium, fluoroscopy time, or radiation dose. Patients with CCT/3D-TEE had a longer hospital stay on average. Besides, there was a different incidence of renal diseases (49% for 3D-TEE versus 27% for CCT/3D-TEE; p < 0.001). The number of periprocedural adverse events was comparable. A device-related thrombus occurred three times in each group, and the peri-device leaks reported were similar.
Conclusion: A preprocedural CCT does not decrease major adverse events or improve outcome in patients undergoing LAAC.
Atrial fibrillation (AF) occurs in 1-2% of the population in western countries and has a higher prevalence in men and older subjects [1-3]. One of the most feared complications in patients with AF is thromboembolism [5]. Approximately 90% of all thrombi develop in the left atrial appendage (LAA) [4]. Therefore, it is not surprising that one in five strokes are caused by AF, and 80% of all strokes are of an ischemic etiology [6, 7, 37].
In order to reduce the risk of strokes, oral anticoagulation with vitamin K antagonists (VKA) and new oral anticoagulants (NOACs) is a validated treatment [8, 9]. Nonetheless, the use of oral anticoagulants (OACs) increases the risk of intracerebral and gastrointestinal bleeding [10-13]. Hence the use of the clinical scores, HAS-BLED and CHA2DS2-VASc score, help to balance the risk of strokes and major bleeding in patients with AF [14, 15]. Interventional closure of the LAA (LAAC) has been shown to be a valid alternative in patients with a contraindication against OACs [16, 17].
In the process of device implantation, planning and preprocedural imaging of the LAA is important.
There are currently two main imaging techniques to assess the LAA before LAAC:
Two-dimensional and three-dimensional (2D/3D)-transesophageal echocardiography (TEE) and cardiac computed tomography (CCT) [19].
3D-TEE is used generally for preprocedural planning and periprocedural intervention, to assess the geometry and size of the LAA and, at most, predict the correct device size [22-24]. It was shown to be superior to 2D-TEE with regard to determining the LAA orifice area/size [24] and LAA occluder size [28]. One study postulated that LAA measurements obtained using real time 3D-TEE showed smaller values than those obtained with CCT [26] and another study found that 3D-TEE was inferior at defining the ostial perimeter and correct occluder size, as compared to CCT [27].
Nonetheless, 3D-TEE imaging allows the LAA to be well visualized before, during, and after the procedure [25].
Cardiac computed tomography (CCT) has been shown as a valid imaging modality to detect LAA thrombi [23], to describe the LAA morphology, and to calculate the predicted device size for the LAAC [20, 21]. However, CCT imaging of the LAA is associated with nephrotoxic risks from the intravenous contrast dye and radiation exposure [29]. Importantly, it was demonstrated that there is a better agreement of the actual diameters and perimeters compared with device diameters and perimeters, i.e. the device fits the dimensions better, for CCT compared to TEE [27, 30].
There are only a few studies that have examined the influence of preprocedural CCT and TEE versus TEE alone, in terms of procedure time, contrast use, correct device size and number of devices utilized. Two small studies have shown a significant reduction in procedure time and anesthesia time, a greater accuracy in device selection, and an absence of peri-device leaks in the group that received a preprocedural CCT [30, 31]. However, data on the influence of preprocedural CCT, concerning the periprocedural and long-term transesophageal echocardiographic outcome, are scarce.
The aim of our study was to compare the influence of preprocedural planning of the LAAC with 3D-TEE and CCT versus 3D-TEE alone, in patients who underwent LAAC with the Amplatzer Cardiac Plug (ACP) and Amulet device, to assess the periprocedural outcome and the long-term transesophageal echocardiographic outcome.
2. Materials and Methods
In this retrospective study, we collected data from a total of 343 consecutive patients with AF and contraindication to effective OAC, who underwent a LAAC procedure with the ACP or AMPLATZER Amulet between September 2009 and December 2019, were appraised and analyzed [45]. The main focus of this study was to compare the impact of CCT versus TEE in terms of preprocedural planning and the clinical outcome of the LAAC: Group 1 had 3D-TEE and CCT (n=176) versus Group 2 had 3D-TEE (n=167) alone. In both groups, clinical characteristics and patient demographics as well as procedural performance, clinical outcome, and echocardiographic follow-up data were collected and statistically contrasted with each other.
2.2 Preprocedural imaging
The 3D-TEE was performed by using a GE Vivid E9 BT12 cardiovascular ultrasound system, at least 24 hours prior to the LAAC procedure. The main aim of the imaging was to exclude intracardial thrombus and to assess three-dimensional images of the LAA. By using the zoom mode from pyramidal data sets, LAA images were recorded by using one-beat acquisition at end-expiration with a resolution of 18 to 21 beats per second [32]. The objective of images obtained was to display the landing zone (LZ) to its full extent and to create a three-dimensional visualization of the LAA by slicing the pyramidal data sets along x, y, and z axes [32].
The imaging data was subsequently analyzed with the GE EchoPAC BT12 software using the 12-channel multislice mode, thus helping to display the LAA in a three-dimensional way. With the help of a cross-sectional view, the perimeter, area, and maximal/ minimal diameter (D max, D min) of the LZ was measured, which is defined as a level plane from the left circumplex coronary artery to the roof of the LAA, approximately 10 mm inward from the peak of the rim that separates the LAA and the left superior pulmonary vein [32]. The mean diameter (D average) was derived from the perimeter (Dper) using the formula: Dper = P/π.
Further details on the use of 3D-TEE images were previously described [23, 32].
2.2.2 Cardiac CT (CCT)
CCT scans were performed by Siemens Somatom Definition Flash (Siemens Healthcare CT Systems, Forchheim, Germany), a dual source 256-slice CT scanner, at least 24 hours prior to the LAAC procedure and usually on the same day as the TEE. The first preprocedural images were generated in September 2012.
The focus for the evaluation of the CCT images was detecting/excluding a thrombus in the LAA, assessing the size of the landing zone, and therefore, predicting the size of the device needed, and finally, identifying the LAA anatomy [37]. Imeron® 350 (350 mg iodine/ml) was intravenously administered as the contrast agent, with an average of 40–100 ml given per scan depending on the patient characteristics, most notably their weight and renal function [40].
The images were made with a prospective ECG gating technique that considers the R-R-interval [40]. The recorded images of the LAA were subsequently analyzed by 3mensioTM, an LAA workflow assistant (Pie Medical Imaging, Maastricht, The Netherlands).
By using the trans-axial images, the circumflex artery, the pulmonary vein ridge, and the LAA ostium were displayed [27]. With the help of the multiplanar reconstruction (MPR) view, a plane from the level of the circumflex artery to 10 mm below the pulmonary vein ridge was drawn, which defined the landing zone. Furthermore, the landing zone was displayed in a cross-sectional view and the diameter calculated from the perimeter was assigned as described above.
Elaborate descriptions of the preprocedural CCT were published previously [27, 37, 38, 39, 40].
2.3 Implantation of the Device
The LAAC implantation process was performed in all patients under general anesthetic. The execution of the implantation procedure was made by using contrast angiography and periprocedural TEE, using the GE Vivid E9 BT12 [18].
The device selection was made based on the measurements of the maximum diameter of the LZ, as described above, and contrast angiography, as recommended by the manufacturer´s instructions (AMPLATZER Cardiac Plug, AMPLATZER Amulet, Left Atrial Appendage Occluder Instructions for Use, St. Jude Medical, Minnesota, USA) [18].
2.4 Angiographic Assessment of the Implantation Procedure
The time from the beginning of the procedure until the extubation of the patients, the fluoroscopy time in minutes, the radiation dose (cGy*cm²), and the amount of contrast dye given in milliliters were registered by using the DAVID hemodynamic software (Metek, Germany) [18]. Beyond this, procedural success as well as device resizing were assessed.
2.5 Periprocedural Adverse Events
With respect to the VARC (Valve Academic Research Consortium) criteria and the Munich consensus document [35, 36], major adverse events (MAEs) included periprocedural mortality, strokes, systemic embolism, myocardial infarction, cardiac tamponade, major bleeding, device embolization, and need for surgery. Furthermore, other adverse events such as TIA, air embolism, vascular complications, as well as acute kidney injuries were assessed and evaluated.
The primary endpoint was defined as the clinical outcome (MAEs and other adverse events) of the LAAC. The secondary endpoint focused on the device-related outcome (device-related thrombus and peri-device leakage) in the echocardiographic follow-up of the patients.
2.6 Echocardiographic Follow-Up of the Patients
Almost every patient received one to three follow-up TEEs in a period from one month to two years in order to track the position of the device, thrombus formation, and peri-device leaks using Echo color Doppler and multiple TEE views, as previously suggested [36].
Leaks were defined, with regard to the width of the color jet-flow, as a minor leak (< 1mm), moderate leak (1-3 mm), major leak (> 3 mm), or severe leak (multiple jets or free flow) [18].
2.7 Statistical analysis
Continuous variables are described as the mean ± standard deviation (SD) and were analyzed via paired or unpaired Student’s t-tests, if distribution was normal.
Categorical variables are described as absolute numbers and percentages. The Chi-square test was used to compare categorical variables.
Statistical significance was considered as a two-tailed probability value <0.05. Statistical analyses were performed with SPSS version 26 (IBM Corp., Armonk, NY, USA).
3.1 Patient characteristics
343 consecutive patients who underwent LAAC, from September 2009 to December 2019, were enrolled in this study. 176 patients received a preprocedural CT and a 3D-TEE, 167 patients received exclusively a preprocedural 3D-TEE. Baseline patient characteristics are shown in (Table 1).
Most patient characteristics did not differ significantly between the two groups. However, there was a significant difference in the HASBLED score with 4.1 ± 1.1 for the 3D-TEE group and 3.9 ± 1.01 for the CT/3D-TEE group (p = 0.05). Whereas, the CHA2DS2-VASc score was similar between the groups (4.57 ± 1.48 for 3D-TEE versus 4.72 ± 1.62 for CT/3D-TEE; p = 0.21).
Medications were well-balanced between the groups. However, 122 (73%) patients of the 3D-TEE group and 109 (62%) patients of the CT/3D-TEE group (p = 0.03) received diuretics. The corresponding values for ACE inhibitors were 48 (29%) patients for the 3D-TEE and 71 (40%) patients for the CT/3D-TEE (p = 0.02) group.
Furthermore, there were more smokers in the 3D-TEE guided group (n = 56 (34%) for 3D-TEE versus n = 37 (21%) for CT/3D-TEE, p = 0.01).
Not surprisingly, the 3D-TEE guided group had a higher prevalence of renal disease (n = 81 (49%) for 3D-TEE versus n = 47 (27%) for CT/3D-TEE; p < 0.001). This finding was also reflected by the creatinine levels (1.59 ± 1.0 mg/dl for 3D-TEE versus 1.21 ± 0.88 mg/dl for CT/3D-TEE; p < 0.001).
3.2 Indications for LAAC
In both groups, more than a half of all patients has had a previous major bleeding event (n = 93 (56%) for 3D-TEE versus n = 89 (51%) for CT/3D-TEE; p = 0.34), which was the most important indication for LAAC (listed in Table 2) in this study. Although, there were significantly more patients in the 3D-TEE guided group with previous gastrointestinal bleeding (n = 55 (33%) for 3D-TEE versus n = 41 (23%) for CT/3D-TEE; p = 0.047).


3.3 Data
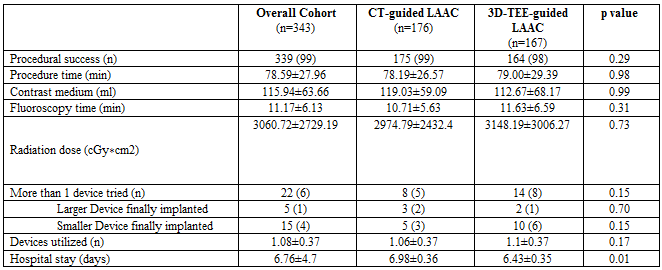
339 of 343 LAAC procedures were successful, resulting in an overall success rate of 99%. There was no significant difference for the success rate between the CT and 3D-TEE guided group (n = 175 (99%) for CT/3D-TEE versus n = 164 (98%) for 3D-TEE; p = 0.29).
The failed attempt at device implantation in the CT/3D-TEE guided group was due to a complicated anatomy of the LAA. In the 3D-TEE guided group, the reasons for the failure of the LAAC procedure were:
1. periprocedural death due to pulseless electrical activity,
2. A complicated LAA anatomy, and
3. An unsuccessful puncture of the atrial septum as a result of a teflon patch of the interatrial septum after cardiac surgery.
There was no significant difference for both groups concerning the procedure time, the amount of contrast medium used, the fluoroscopy time, or the radiation dose.
Importantly, there was also no significant difference in the number of devices that needed to be resized in the 3D-TEE guided group (n = 14 (8%) versus n = 8 (5%) for CT/3D-TEE (p = 0.15).
However, patients who received a CCT before LAAC stayed longer in the hospital than those patients without CCT (6.43 ± 0.35 days for 3D-TEE versus 6.98 ± 0.36 days for CT/3D-TEE; p = 0.01).
3.4 Adverse events
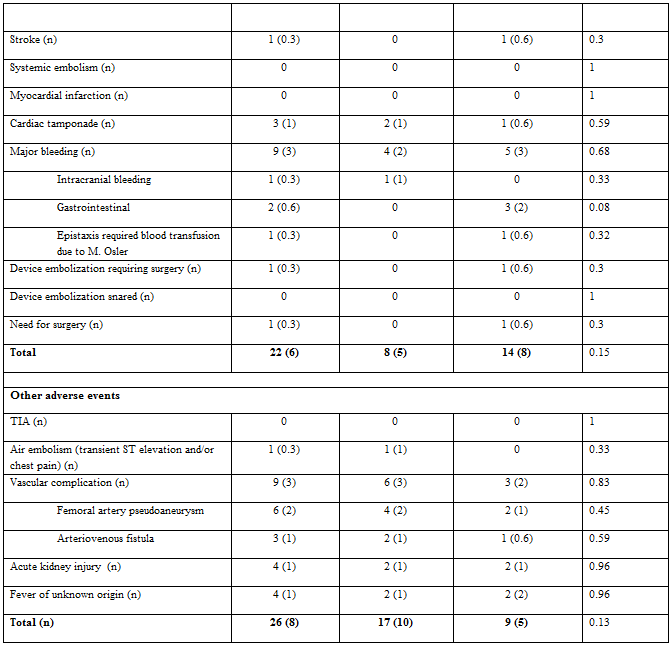
Twenty-two (6%) of 343 consecutive patients who underwent LAAC suffered from a major adverse event. Of these, 14 patients (8%) from the 3D-TEE guided group and 8 patients (5%) from the CT/3D-TEE guided group were affected (p = 0.15).
Three accumulated deaths were observed in both groups. One patient of the CT/3D-TEE guided group died after a cardiac tamponade following LAAC and a volume deficiency shock after cardiopulmonary resuscitation. Of the two reported deaths in the 3D-TEE group, one was caused by a pulseless electrical activity during the LAAC, and the other patient had a device dislocation after the intervention and died of a bleeding complication following the operation to remove the device. There was no statistical difference between the two groups regarding deaths (p = 0.53).
Major bleeding after LAAC appeared in five cases (3%) in the 3D-TEE group and four cases (2%) in the CT/3D-TEE group with no statistical difference (p = 0.68). Those events were divided into three (2%) gastrointestinal bleedings, one (0.6%) epistaxis due to M. Osler and one (0.6%) inguinal bleeding after puncture in the 3D-TEE group. In the CT/3D-TEE group, there was one (0.6%) intracranial bleeding, one (0.6%) hemorrhagic pericardial tamponade requiring one erythrocyte concentrate, one (0.6%) epistaxis, and one (0.6%) traumatic hard palate bleeding, that were defined as major bleeding events.
Two cases of acute kidney injuries were reported in each of the groups after LAAC, with no significant difference (p = 0.96).
3.5 Echocardiographic follow up
Of all the patients that underwent LAAC in this study, 288 (84%) patients received at least one follow up 3D-TEE, at the earliest, one month after the procedure. Those were divided in 154 (53%) patients for the CT/3D-TEE guided group and 134 (47%) patients for the 3D-TEE guided group (p = 0.09).
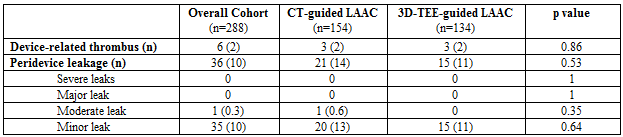
In each group, three cases (1.8% for 3D-TEE and 1.7% for CT/3D-TEE; p = 0.86) of device-related thrombi were detected (Table 5).
Furthermore, there were no significant differences in terms of minor leaks (n = 15 (11%) for 3D-TEE versus n = 20 (13%) for CT/3D-TEE; p = 0.64) or moderate leaks (n = 0 for 3D-TEE versus n = 1 (0.6 %) for CT/3D-TEE; p = 0.35). There were no major leaks in either group.
339 of 343 LAAC procedures were successful, resulting in an overall success rate of 99%. There was no significant difference for the success rate between the CT and 3D-TEE guided group (n = 175 (99%) for CT/3D-TEE versus n = 164 (98%) for 3D-TEE; p = 0.29).
The failed attempt at device implantation in the CT/3D-TEE guided group was due to a complicated anatomy of the LAA. In the 3D-TEE guided group, the reasons for the failure of the LAAC procedure were:
1. periprocedural death due to pulseless electrical activity,
2. A complicated LAA anatomy, and
3. An unsuccessful puncture of the atrial septum as a result of a teflon patch of the interatrial septum after cardiac surgery.
There was no significant difference for both groups concerning the procedure time, the amount of contrast medium used, the fluoroscopy time, or the radiation dose.
Importantly, there was also no significant difference in the number of devices that needed to be resized in the 3D-TEE guided group (n = 14 (8%) versus n = 8 (5%) for CT/3D-TEE (p = 0.15).
However, patients who received a CCT before LAAC stayed longer in the hospital than those patients without CCT (6.43 ± 0.35 days for 3D-TEE versus 6.98 ± 0.36 days for CT/3D-TEE; p = 0.01).
Twenty-two (6%) of 343 consecutive patients who underwent LAAC suffered from a major adverse event. Of these, 14 patients (8%) from the 3D-TEE guided group and 8 patients (5%) from the CT/3D-TEE guided group were affected (p = 0.15).
Three accumulated deaths were observed in both groups. One patient of the CT/3D-TEE guided group died after a cardiac tamponade following LAAC and a volume deficiency shock after cardiopulmonary resuscitation. Of the two reported deaths in the 3D-TEE group, one was caused by a pulseless electrical activity during the LAAC, and the other patient had a device dislocation after the intervention and died of a bleeding complication following the operation to remove the device. There was no statistical difference between the two groups regarding deaths (p = 0.53).
Major bleeding after LAAC appeared in five cases (3%) in the 3D-TEE group and four cases (2%) in the CT/3D-TEE group with no statistical difference (p = 0.68). Those events were divided into three (2%) gastrointestinal bleedings, one (0.6%) epistaxis due to M. Osler and one (0.6%) inguinal bleeding after puncture in the 3D-TEE group. In the CT/3D-TEE group, there was one (0.6%) intracranial bleeding, one (0.6%) hemorrhagic pericardial tamponade requiring one erythrocyte concentrate, one (0.6%) epistaxis, and one (0.6%) traumatic hard palate bleeding, that were defined as major bleeding events.
Two cases of acute kidney injuries were reported in each of the groups after LAAC, with no significant difference (p = 0.96).
3.5 Echocardiographic follow up
Of all the patients that underwent LAAC in this study, 288 (84%) patients received at least one follow up 3D-TEE, at the earliest, one month after the procedure. Those were divided in 154 (53%) patients for the CT/3D-TEE guided group and 134 (47%) patients for the 3D-TEE guided group (p = 0.09).
In each group, three cases (1.8% for 3D-TEE and 1.7% for CT/3D-TEE; p = 0.86) of device-related thrombi were detected (Table 5).
Furthermore, there were no significant differences in terms of minor leaks (n = 15 (11%) for 3D-TEE versus n = 20 (13%) for CT/3D-TEE; p = 0.64) or moderate leaks (n = 0 for 3D-TEE versus n = 1 (0.6 %) for CT/3D-TEE; p = 0.35). There were no major leaks in either group.

Table 5. Prevalence and severity of peridevice leaks at transesophageal echocardiographic follow up
LAAC is an established alternative to oral anticoagulation treatment in patients with AF and contraindications against OACs [46]. In order to achieve an effective procedure for each patient, in terms of present and long-term implantation success and a reduction of adverse events, we retrospectively investigated the influence of CCT as an additional preprocedural imaging modality besides the commonly utilized 3D-TEE.
In comparison to the ACP multicenter registry [41], we had a similar overall procedural success rate in our study (97.3% vs 98.8%) and periprocedural MAE rate (5% vs. 6.4%). In concordance with our results, Koskinas et al. [42] reported MAEs of 5.8% in 500 consecutive patients.
An important finding of our study was that we did not find a difference in the procedural success rate between patients who underwent a CCT-planned strategy for LAAC and patients with a 3D-TEE-only guided strategy (99% versus 98%). Furthermore, we did not detecthigher first-device accuracy in the CCT/3D-TEE group (94.9%) than in the 3D-TEE group (91%). In addition, the overall number of devices used was not different between the CCT/3D-TEE and 3D-TEE only groups (1.06 ± 0.37 for CCT vs. 1.1 ± 0.37 for 3D-TEE; p = 0.17).
In contrast, a much smaller study by Eng et al. [44], which randomized 24 patients to undergo LAAC using either 2D-TEE or 3D-CT for implanting WATCHMAN™ devices, found a higher procedural success rate in the 3D-CT than in the 2D-TEE group (100% vs 92%). Furthermore, this study showed that the accuracy for first device selection and the number of devices used was significantly better for 3D-CT than 2D-TEE (92% vs. 27% and 1.33 ± 0.7 vs. 2.5 ± 1.2, respectively). The difference between our findings and the study by Eng et al. may be explained by the smaller study group, different device used, and by the use of 2D-TEE, which is much less accurate than 3D-TEE [28, 32].
Dutcher et al. [31] compared a CT-guided and TEE-guided strategy in 154 consecutive patients (CT n = 76 vs. TEE n = 78) who received the WATCHMAN device. The authors of this study reported a significantly better accuracy rate concerning first device selection in the CT group with 86.7% for the CT-guided group vs 75.6% for the TEE group (p = 0.041). However, the difference between the groups was much smaller than in the study by Eng et al. [44]. Dutcher et al. also reported procedure times for the different groups. They observed significantly shorter procedure times in the CT group (33.6 min vs 46.5 min for TEE). In our study, the procedure time did not differ between the CCT/3D-TEE and 3D-TEE only groups.
We found in our study that fluoroscopy time and radiation doses did not differ between patients in the CCT/3D-TEE and in the 3D-TEE group. An interesting but small study of 24 patients receiving the WATCHMAN device by Obasare et al. [30] used a preprocedural CT to produce a latex model of the LAA using 3D printing (n = 14) and compared that to preprocedural 2D-TEE imaging. The authors of this study reported of a significantly reduced procedure time (70 ± 20 vs. 107 ± 53 min for 2D-TEE, p = 0.03) and fluoroscopy time (11 ± 4 vs. 20 ± 13 min for 2D-TEE, p = 0.02) for preprocedural CT. Unfortunately, there are some limitations concerning the comparisons of our study to Dutcher et al. and Obasare et al. as they both used the WATCHMAN device, were much smaller, and applied different imaging concepts, including 2D-TEE, which is inferior to 3D-TEE.
4.2 Long-term echocardiographic outcome
Landmesser et al. [43] showed in a large prospective Amplatzer Amulet observational study an adequate occlusion (< 3mm jet) of the appendage in 98.2% and detected a device thrombus in only 1.5% of 673 patients in the TEE follow-up, 67 ± 23 days after LAAC. Based on the definition of major leaks (jet-flow > 3 mm) by the Munich consensus document [40], we did not detect any major leaks, although we had one (0.6%) moderate and 35 (10%) minor leaks in the first follow-up TEE, at the earliest one month after LAAC in 288 available patients. However, our device-related thrombus rate (2.1%) was similar to the rate reported by Landmesser et al [43].
Importantly, in our study we could show that an absence of peri-device leaks was not statistically different between the 3D-TEE guided group and the CCT/3D-TEE group (88.8% vs. 86.4%). It is interesting that this finding is in concordance with the finding of Obasare et al., who reported an absence of peri-device leaks in 92% of patients who received a CT-based 3D-printed model.
Although patient characteristics were distributed predominantly equally in both groups, there were significantly more patients in the 3D-TEE guided group with a decreased renal function and a known renal disease. This is probably due to the selection bias of a non-randomized study, since the use of contrast agent during CCT can provoke acute renal failure or deteriorate renal function, in particular in patients with known renal disease, so it is likely that these patients were selected against for CCT.
Nevertheless, in our study, 27% of patients received a preprocedural CCT even though they had known renal disease. Interestingly, only two patients (1%) suffered from an acute kidney injury during their hospital stay in the CCT/3D-TEE arm, which was also the case in the 3D-TEE only guided group (two cases (1%)). All of these patients regained their original renal function during the hospital stay, under continued renal-protection measures. In this respect, it is important to note that in our study, patients in the CCT/3D-TEE arm did not need less contrast agent than in the 3D-TEE arm during the procedure (120 ml versus 112 ml). Hence, a CCT-guided strategy does not save contrast agent during the procedure.
Moreover, patients with an additional preprocedural CCT had a significantly longer hospital stay (6.4 ± 0.4 days for 3D-TEE alone versus 7 ± 0.4 days for CT/3D-TEE; p = 0.01) due to the fact that the CCT was performed one day before implantation of the device.
In conclusion, we did not find any difference between the preprocedural 3D-TEE and CCT/3D-TEE guided groups with respect to the primary endpoint, which was defined as the clinical outcome of the LAAC, or the secondary endpoint consisting of the echocardiographic follow-up.
In consideration of our results, we would suggest that a preprocedural CCT may be avoided before planning a LAAC, as we did not detect a decrease of MAEs or improved outcome. Moreover, the addition of a CCT leads to higher costs and a potentially longer hospital stay.
The most important limitation of our study is its retrospective design. However, we only included consecutive patients. Furthermore, it was regarded as potentially difficult to randomize patients with advanced renal dysfunction to the CCT/3D-TEE group.
In our study, 3D-TEE was used for LAAC implantation, which was performed by experienced operators. Hence our results cannot be applied to centers that use only 2D-TEE for LAAC implantation guidance.
Conflict of Interest Disclosures:
The authors have no conflicts of interest to declare.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
