
Case Report | DOI: https://doi.org/10.31579/2640-1053/087
*Corresponding Author: Refka Frioui, Department of Dermatology, Farhat Hachad Hospital, Ibn Jazzar, 4000 Sousse, Tunisia.
Citation: R Frioui, A Ghannem, R Frioui, M Tabka, B Sriha, C Belajouza, M Denguezli. (2021) Carcinoma en cuirasse associated to zosteriform metastasis from breast adenocarcinoma. J.Cancer Research and Cellular Therapeutics. 5(4); Doi: 10.31579/2640-1053/087
Copyright: © 2021 Refka Frioui, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 June 2021 | Accepted: 14 June 2021 | Published: 28 July 2021
Keywords: breast adenocarcinoma; carcinoma en cuirasse; zosteriform metastasis; controlateral carcinoma
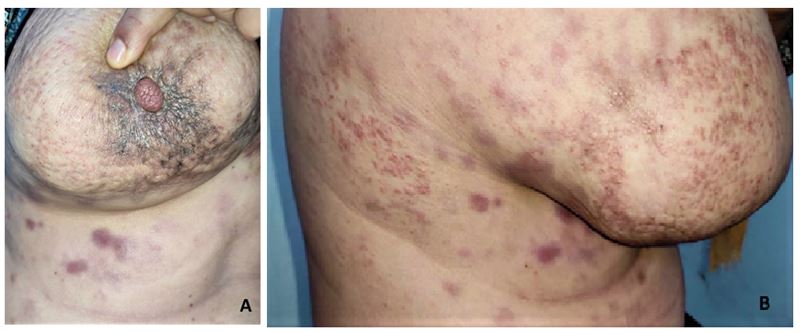
We report an original case of carcinoma en cuirasse associated with zosteriform metastasis. A 40-year-old woman presented to our department with painful erythematous lesions. She had a history of invasive ductal carcinoma of the left breast. Numerous erythematous, papules and whitish vesicles were present over the right side of the chest in a dermatomal distribution with indurated coalescent plaques. Biopsy revealed metastatic carcinoma of breast origin. Breast mammography showed suspicious right nodule. Controlateral breast carcinoma with CM was diagnosed. CM show a wide range of clinical manifestations. Carcinoma en cuirasse, is a very rare form of metastatic cutaneous breast cancer. It is characterized by diffuse sclerodermatous induration of the skin. Zosteriform metastasis is also rarely seen. It may be distributed along dermatomeres in a variety of clinical patterns, including nodular, papulovesicular, or vesiculobullous. In our case, the zosteriform metastasis occurred in the contralateral site. It announced the developing of contralateral breast cancer.
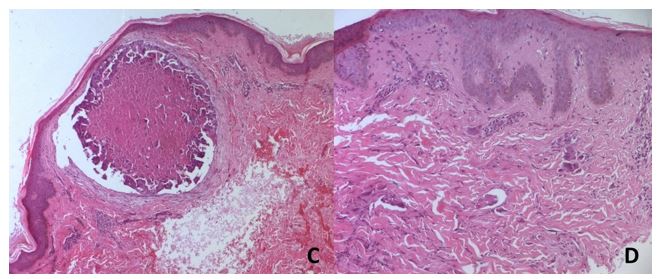
A 40-year-old woman was referred to our department with painful erythematous papules grouped on the right side of the trunk of two-month duration. She had a history of left infiltrating ductal carcinoma 3 years back, treated with chemotherapy, mastectomy and radiotherapy. On examination, numerous firm erythematous and whitish clustered papules were present over the right side of the chest in a dermatomal distribution (T4–T6) with peaud'orangeappereance (Figure1). The underlying skin was indurated. Many diffuse sclerodermiform and erythematous plaques were also present. There was a palpable mass in the right mammary gland. Two biopsies were performed from a papule and an indurated plaque revealing same histologic features: a dense dermal infiltration of malignant epithelial cells delimiting cribriform clusters with lymphangitic carcinomatosis.Collagen densification was also seen (Figure2). Microbiopsy of the breast nodule confirmed the malignant origin. Computed tomography scan showed significant bilateral pleural effusion. No distant metastasis was detected. Controlateral BC with CM was finally diagnosed. The patient was started on palliative chemotherapy after a multidisciplinary team meeting.
Cutaneous metastasis (CM) are rare malignancies appearing as tumor cells spreading over skin directly, hematogenous or lymphatically from primary tissue [1, 2]. Breast cancer (BC) is the first internal malignancy associated with CMs of different clinical presentations [2]. CMs in patients with BC occur in 23,9%.3 Erythematous papules and nodules are the most common presentation (80% of cases) [4]. Less commonly, atypical variants of skin involvement in BC can mimic common processes: erysipelas (carcinoma erysipeloides), alopecia areata (alopecia neoplastica), lymphangioma circumscriptum and cutaneous vasculitis (carcinoma teleangiectaticum) [4]. CC and ZM, presented here, resembling morphea and herpes zoster respectively are extremely rare. In those exceptional cases, only histology can make the diagnosis which often resembles the primary cancer.
CC is seen in only 3% of patients with CMs from BC [4]. It is characterized by erythematous indurated plaques with diffuse sclerodermatous induration of the chest wall skin [3]. It is most commonly linked with local recurrence of BC following mastectomy, chemotherapy, or radiotherapy, as in our case, but it can also be a clinical presentation of a primitive tumor [4]. CC is characterized histologically by dense fibrosis with few neoplastic cells and decreased vascularity, making it highly resistant to chemotherapy [3]. This form of CM was rarely associated with other visceral malignancies [5].
ZM is a rarely seen subtype with only a few hundred casesin the literature, among them 12 cases due to BC [6]. It may be distributed along dermatomes in various clinical patterns, including nodular, papulovesicular, or vesiculobullous [3]. Several theories have been proposed to clarify the pathogenetic mechanism of zosteriform dissemination. It has been postulated to occur as a Koebner response to recent herpes zoster [6]. Our patient did not report any skin lesion over the area previously. ZM may also be generated by the diffusion of tumor cells from the perineural lymphatic vessels [3]. This is likely to be the cause in our patient having lymphangitic carcinomatosis in histology. Diagnosis of ZM can be challenging, resulting in initial misdiagnosis. Occurring in oncologic immunosuppressive patients, it can be confused with herpes zoster infection. Definite diagnosis is made on microscopic examination. In our case, ZM occurred in the contralateral site, revealing a contralateral BC. Association of CC and ZM has not been reported yet.
To conclude, CM should be included in the differential of potentially benign lesions in patients with neoplastic disease history.
The authors declare having followed the protocols in use at their working center regarding patients’ data publication.
Obtained.
All authors report no conflict of interest.
No funding.
Authors were responsible for the minimal costs involved in this article.
None
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
