
Case report | DOI: https://doi.org/10.31579/2693-4779/025
1 East Sussex Healthcare NHS Trust, East Bourne, United Kingdom
*Corresponding Author: Anurup Kumar, East Sussex Healthcare NHS Trust, East Bourne, United Kingdom.
Citation: Anurup Kumar. (2021) Capnocytophaga canimorsus Meningitis-Diagnosis with 16S rDNA PCR when Conventional Methods Failed to Identify the Causative Agent. Clinical Research and Clinical Trials. 3(2); DOI:10.31579/2693-4779/025
Copyright: © 2021, Anurup Kumar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 February 2021 | Accepted: 27 April 2021 | Published: 30 April 2021
Keywords: capnocytophaga canimorsus meningitis; 16S rDNA PCR; causative agent
Meningitis whether bacterial or viral, poses many challenges to clinicians as the causative agent is often not found. According to guidelines, it is standard to start empiric treatment before a Cerebrospinal Fluid (CSF) sample is obtained. Meningitis, if not diagnosed and treated early, can lead to high morbidity and mortality rates with serious neurological sequelae. While the most common cases of bacterial meningitis are related to Streptococcus pneumoniae and Neisseria meningitidis, this clinical case report found a rare case of meningitis caused by a zoonotic pathogen, Capnocytophaga canimorsus; a commensal found as part of the normal flora of dogs and cats. This rare organism was identified with the help of broad range 16S ribosomal DNA Polymerase Chain Reaction (rDNA PCR), an emerging technique that is now increasingly useful in rapid diagnosis especially if the offending agent is not timely identified and conventional methods have failed, making diagnosis and management difficult for physicians.
Meningitis whether bacterial or viral, poses many challenges to clinicians as the causative agent is often not found. According to guidelines, it is standard to start empiric treatment before a Cerebrospinal Fluid (CSF) sample is obtained. Meningitis, if not diagnosed and treated early, can lead to high morbidity and mortality rates with serious neurological sequelae. While the most common cases of bacterial meningitis are related to Streptococcus pneumoniae and Neisseria meningitidis, this clinical case report found a rare case of meningitis caused by a zoonotic pathogen, Capnocytophaga canimorsus; a commensal found as part of the normal flora of dogs and cats. This rare organism was identified with the help of broad range 16S ribosomal DNA Polymerase Chain Reaction (rDNA PCR), an emerging technique that is now increasingly useful in rapid diagnosis especially if the offending agent is not timely identified and conventional methods have failed, making diagnosis and management difficult for physicians
Epidemiology
Capnocytophaga canimorsus is a rare species that causes severe and often fatal infections in humans. The incidence in general population is very low. In a national survey carried out in the Netherlands, an incidence ratio of 0.67 cases per million per year was present [4]. As part of the normal flora, it is commonly present in the oral cavities of 67 to 86% of dogs and 55-84% of cats [5, 6].
Capnocytophaga canimorsus, (C. Canimorsus), historically known as ‘dysgonic fermenter 2 (DF-2)’ due to its slow-growing, fastidious and fermenting properties was first observed in 1976 by RA Bobo and EJ Newton (1976).). It was isolated from a patient who was bitten by a dog and consequently developed sepsis and meningitis [7, 8]. It is a gram negative, capnophilic (carbon-loving), catalase- and oxidase+ anaerobic bacillus and is one of 9 isolated species, including C. ochracea, C. gingivalis, C. cynodegmi, C. hemolytica, some of which are found inhabiting the human oral cavity [9]. 3 serovars (variants) of C. Canimorsus (A, B and C) are known to cause nearly 90% of disease in humans [10].
Capnocytophaga canimorsusus tillses sugars from glycoproteins in host cells. It prevents macrophages from killing bacteria by blocking release of Tumour Necrosis Factor alpha and various Interleukins including Iinterleukin-1, 6 and 8. It also has a unique lipo-polysaccharide capsule that inhibits complement-mediated fixation and eventual phagocytosis by macrophages – all contributing to its capacity of evasion from the human immune system
Canimorsus infection can present as sepsis, endocarditis, cellulitis, gangrene of digits, purpurafulminans, acute abdomen and rarely meningitis, all following a dog bite. However, contact in the form of licking or superficial scratches have also been reported to transmit the organism
Infection with this bacterium is typically seen in asplenic or immune-compromised patient.As the bacterium is incredibly fastidious and cultures slowly, it is often difficult to identify with conventional methods of culture and gram staining, thus making the diagnosis problematic.
Conventional techniques used in the identification include slow culture on blood-agar [18]. However, now a newer technique, 16S rDNA PCR or broad range gene sequencing is becoming increasingly vital. Especially in cases where the clinical suspicion for meningitis remains high and the causative organism remains elusive.
C. Canimorsus is mostly susceptible to Penicillin, Cephalosporins and Carbapenems. Some resistant strains of Capnocytophaga that produce class D beta-lactamase respond well to Clindamycin [19].
This clinical case report a case of meningitis caused by C. canimorsus in a woman with no known risk factors, in whom 16S rRNA gene sequencing aided identification of the pathogen, when conventional methods like culture and quantitative PCR failed.
A 70-year-old female with no prior history of immune suppression presented to the Emergency department with a three week history of tinnitus, ‘fullness’ in the ears and one day history of severe headache, hoarseness of voice, hearing loss and worsening ataxia. At the time of admission, the patient was found to be photophobic and had severe hearing impairment. Clinically, no other neurological abnormalities could be elicited. The patient had a previous history of breast cancer and head injury following a traumatic accident. She also had chronic issues with her balance and gait. This was attributed to the superficial siderosis found on imaging, possibly following the accidents that she had suffered earlier in her life.
Considering the presentation, the patient was immediately isolated and empirically treated with Intravenous Acyclovir and Ceftriaxone in line with the protocol for treatment of cases of suspected meningitis of unknown aetiology.
An urgent CT Scan of Head did not show any acute pathology, although it did revealed significant atrophy of Cerebellar Vermis which explained the chronic issues with gait. A Lumbar puncture was then undertaken, and the Cerebro-spinal fluid (CSF) analysis revealed the following: Glucose 1.4 (serum: 6.7); WCC: 96 (polymorphs 20% and lymphocytes: 80%); Protein: 2.75; Lactate: 7.3; LDH: 191 (Table 1) – theseresults were not very typical of bacterial meningitis as it did not show predominant polymorph pleocytosis.
Both blood and CSF Cultures failed to grow any organism, hence treatment was continued with broad spectrum cover of Intravenous Ceftriaxone. Intravenous Acyclovir was however stopped as per Consultant Microbiologist advice. Quantitative Polymerase Chain Reaction (qPCR) which tests for specific and most common agents like meningo-coccal and pneumo-coccal organisms also came back negative.
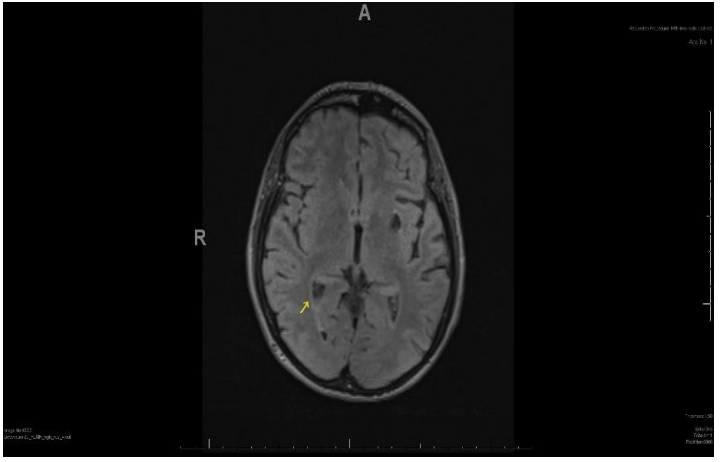
We requested an MRI Head to further guide treatment. It revealed appearances in-keeping with the diagnosis of meningitis. An abnormal signal was noted within the occipital right lateral ventricle, the extra-axial spaces of the frontal convexities and to a lesser degree in the interhemispheric fissure. This was most likely thought to be secondary to infected CSF or pus (Figure 1). The scan also revealed superficial siderosis with cerebellar atrophy (possibly secondary to previous head injuries) further explaining the pre-existing ataxic gait.
After approximately 10 days of initiation of treatment, a second CSF sample was sent for analysis, to assess for response. The symptoms had failed to improve during this time. The results revealed signs of active infection with high proteins: 2.64, WCC: 106 and Lact: 4.2 (Table 1). In consistency with the ongoing symptoms of the patient and considering the treatment was continued for further 2 weeks during which the patient reported improvement in symptoms. The causative agent, however was still elusive at this stage. Therefore, to check for response to treatment, a third CSF analysis was undertaken, the results of which were reassuring. By this time Microbiologist alerted us that the causative agent had finally been identified to be Capnocytophaga canimorsus via broad range 16S rDNA PCR technique.
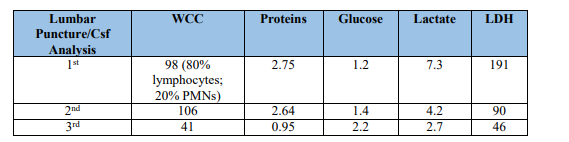
Table 1. WCC, Proteins, Glucose, Lactate and LDH
KEY: WCC- White Cell Count; LDH: Lactate Dehydrogenase; PMNs – Polymorph Neutrophils
Since the results from the 3rd CSF sample had still shown evidence of active infection, we were advised to continue treatment with Meropenem. We observed dramatic clinical improvement and the patient also stated feeling steadier on her feet and started mobilising. The third CSF sample sent earlier tested negative by the 16SrDNA PCR for C. canimorsus. Also,during this time the patient had completed the required course of IV Meropenem and it was at this point the antibiotic therapy was withdrawn. The patient was kept under observation for a few more days to ensure full recovery.
The patient remained well afterwards and was seen by ENT to investigate the cause for the severe hearing impairment. Audiology tests revealed severe and profound Sensory-neural Hearing Loss (SNHL) in her right and left ear, respectively, presumably secondary to the bacterial meningitis considering the acuteness of nature and timeline of events. She was discharged and a follow-up was arranged in clinic.
The main relevant differential diagnosis that were being considered till the agent was identified were of viral/ tuberculous meningitis, leading to the initiation of empirical treatment with an antiviral (Acyclovir) and broad-spectrum antibiotics – (Ceftriaxone). There was also an initial view that the patient might have had a Sub-arachnoid Haemorrhage which was then ruled out by imaging.
The patient was discharged following successful treatment and has been referred for a follow-up in ENT for her hearing impairment and Neurology clinic for her on-going chronic issues with balance. This was believed to be a consequence of her previous brain bleeds and cerebellar atrophy which had worsened due to the acute infection. She preferred to go to a private facility for a period of rehabilitation following her discharge and has remained well.
In 1977, Butler et al. (1977) reported a series of cases with a similar, not yet identified gram negative bacillus, later identified as the same species by the Centre of Disease Control. Since then many cases have been published in literature; however, considering that this bacterial species is only now being recognised mainly due to the advances in molecular techniques. Especially, considering the close relation between man and dog ever since domestication, it may be more common and have an incidence rate much higher than earlier thought [21, 22].
According to available evidence, this organism is most commonly found in the immune-compromised. However, a recent systematic case review undertaken by Hansen and Crum-Cianflone (1977) has disputed this evidence. It showed that out of all cases of C. canimorsus meningitis recorded between 1966 and 2018, only a small minority were found to be immuno-compromised [23]. Out of a total of 37 patients, only 16% had a history of splenectomy and only 5% reported steroid use. Blood cultures were found to be positive only in 54% patients. 70% had positive CSF cultures. PCR was able to identify the organism in 22% of the cases. Antibiotic therapy ranged from 7 to 42 days. Disease prognosis was found to be better for meningitis, with only 1 reported fatality out of the total 37 cases reviewed in the article. 19% of the patients suffered from neurological or physiological sequelae including hearing impairment and ataxia. Over 80% had a history of dog bite or had some form of non-bite exposure such as scratching or licking [24].
Hearing impairment, mostly sensorineural, like what we encountered, is not uncommon and has been reported. Cochlear circulatory dysfunction has been suggested to be linked to sudden sensory-neural hearing loss (SNHL) secondary to bacterial infections which produce lethal levels of cytokines that disrupt the inner ear [25]. Moreover, a case study which analysed eighteen cases of C. canimorsus meningitis revealed that in nearly 50% of the cases, CSF analysis showed predominance of lymphocytes and commonly presented with acute or sub-acute hearing loss [26-28].
A study carried out in Finland during 2000-2017 Reference ???, isolated C. Canimorsus from 73 blood cultures from patients treated at the Helsinki University Hospital. Serotyping by PCR and Western Blot identified 3 serovars or variants (A, B and C) which were found to cause most of the infections in humans (91.8%). The relative prevalence of these serovars was low amongst dog isolates (7.6%) – indicating that these serovars are mostly virulent in humans. The low incidence of infection was due to the low prevalence of the virulent serovars in the oral cavities of dogs. This is despite the fact that C. Canimorsus itself is commonly found in up-to 67-86% of dogs (as previously stated). It further reiterates the fact that virulence of different serovars and not the actual prevalence of C. Canimorsus was what accounts for the rarity of this infection [29, 30].
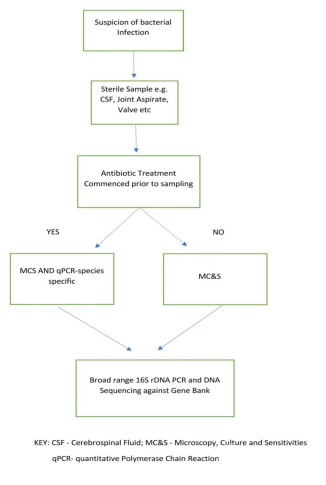
As previously described, C. canimorsus grows very slowly and was difficult to identify via conventional methods of culture. Hence 16S rDNA sequencing is now being increasingly useful in identification of such organisms. While quantitative PCR sequencing targets specific (most common) organisms, 16S rDNA PCR sequencing uses DNA from specimens and checks for a match against a gene bank. Most laboratories initially test samples for common disease-causing organisms. If the initial tests fail to identify the offending agent and the suspicion for an infection remains high, specimens are then tested with broad range 16S rDNA sequencing (Figure 3: Flowchart explaining the process). The commercial techniques lack primers to identify these rare types of organisms. The turn-around time for rDNA PCR sequencing is only about 3- 19 hours (depending on the facilities available) vs. conventional cultures which usually take up to an average of 6 days [31]. Guidelines published by British Infection Association Year??? Also recommend testing via PCR for 16S ribosomal DNA, if blood/CSF cultures or quantitative/pathogen-specific PCR fails to identify the agent [32].

Similarly, another pilot study carried out by Jangsup Moon et al, year ??? revealed that the sequencing could be performed under 3 hours and successfully detected pathogenic bacteria from all samples under study . Their study concluded that this test should be increasingly employed in the future especially in cases like meningitis where disease fatality is high. 16S Amplicon sequencing as it is alternatively known was found to be more sensitive. Moreover, the technique was found to be more sensitive and identified the causative agent even in antibiotic-treated samples. Undeniably, it was an indispensable tool in diagnostic medicine aiding timely identification and targeted treatment [33].
Meningitis is a serious and often fatal infection if not identified and treated early. Mortality rates of untreated cases approach 100 percent. Initial tests apart from CRP and Full blood count include blood cultures, CSF Analysis including biochemistry, gram staining, culture and PCR for specific organisms, most commonly meningococcal- and pneumococcal. According to guidelines published by National Institute of Health and Care Excellence (NICE) Year? Lumbar puncture for a CSF sample was the primary investigation. However, treatment should not be delayed whilst awaiting their results.
IV Ceftriaxone is the antibiotic of choice in suspected cases of bacterial meningitis above 3 months of age. Children younger than 3 months should receive IV Cefotaxime plus either Amoxicillin or Ampicillin. Length of antibiotic therapy varies between 7-14 days. Corticosteroids can be considered in cases where CSF was found to be frankly purulent [34].
Learning Points and Take Home Messages
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
