
Case-Report | DOI: https://doi.org/10.31579/2641-0419/095
1 Nélio Mendonça Hospital, Avenida Luís de Camões, nº 57 – 9004-514 Funchal, Portugal.
*Corresponding Author: Marina Santos., Nélio Mendonça Hospital, Avenida Luís de Camões, nº 57 – 9004-514 Funchal, Portugal.
Citation: Marina Santos., Nuno Santos., Ricardo Rodrigues., Bruno Silva., António Drumond., (2020) Cannabis Induced Vasospasm Complicated By Iatrogenic Coronary Artery Dissection. J, Clinical Cardiology and Cardiovascular Interventions, 3(10); Doi:10.31579/2641-0419/095
Copyright: © 2020 Marina Santos, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 October 2020 | Accepted: 19 October 2020 | Published: 26 October 2020
Keywords: cannabis; marijuana; acute myocardial infarction; coronary vasospasm; iatrogenic coronary dissection
Cannabis is the most abused psychoactive drug in the world. Delta 9-tetrahydrocannibol, the main psychoactive compound in marijuana, acts via the endocannabinoid system to elicit various cardiovascular physiological effects, and has been associated with many adverse cardiovascular effects such as acute coronary syndrome, arrhythmias, and sudden cardiac death. It is important to consider cannabis use as a significant risk factor of myocardial infarction, particularly in individuals with no cardiac risk factors, as delay in management can result in fatal outcomes.
Coronary angiography as the main exam to definitively diagnose or rule out coronary artery disease is usually safe, but complications also occur. Coronary dissection, despite rare, can be extremely difficult to manage and even be fatal. Iatrogenic causes of coronary dissection include catheter tip or guidewire trauma, vigorous contrast injection and angioplasty balloon overinflation.
We present the case of a 41 years old Caucasian woman admitted to cardiology department after an episode of myocardial infarction due to cannabis induced vasospasm. However, the angiography was complicated by iatrogenic coronary artery dissection.
Cannabis, also known as marijuana, is the most common psychoactive drug used worldwide, with rates of consumption expected to rise given increasing legalization for recreational and medical use [1]. Although cannabinoids are the oldest and most widely used drugs, its clinical and pharmacological effects have only been recently studied, with much still unknown about the physiologic and pathologic effects of marijuana. Much of the available data on 9-tetrahydrocannabinol (THC), the main psychoactive ingredient in marijuana, relates to its neurological effects and antiemetic properties, with little on the cardiovascular (CV) effects of THC [2, 3]. However, in the medical literature an association between cannabis and adverse CV events has been demonstrated.
Diverse cases of cannabis-related acute coronary syndrome have been reported, even in people with normal coronary arteries [4-5]. The current literature proposes that marijuana adversely affects the CV system
through three different possible mechanisms – cannabis-induced arteritis, vasospasm, and platelet aggregation [6-8].
A 41 years old Caucasian female presented to the emergency room (ER) with sharp precordial chest pain of three-hour duration accompanied by sweats and nausea. Also, she had an episode of vomit, with pain relief. She was currently taking oral birth control and denied other personal risk factors for ischemic heart disease. Family history was not significant for coronary artery disease or sudden cardiac death.
Upon presentation, patient was hemodynamically stable, and her physical examination was unremarkable. Electrocardiogram (EKG) revealed sinus rhythm at a rate of 98bpm with 1mm ST segment elevations in the V1-V3 and aVR leads and 1mm ST segment depressions in the V4-V6 leads (Figure 1).

Figure 1: EKG reveals sinus rhythm at a rate of 98bpm with QS wave and 1mm ST segment elevations in the V1-V3 and aVR leads and 1mm ST segment depressions in the V4-V6 leads.
High sensitivity cardiac troponin was initially positive (hs-cTnl 1.29mg/mL, reference value <0.014mg/mL) and up trended to a peak of 5.54mg/mL. A transthoracic echocardiography (TTE) showed anterior and apical hypokinesis with an estimated ejection fraction of 45%.
The patient was loaded with aspirin, ticagrelor and heparin and was referred for urgent coronary angiography. The first contrast dye injection revealed normal coronary arteries (Figure 2A).
However, after this injection, an anterograde spiral coronary dissection
appeared, extending from left main coronary artery (LMCA) to the distal portion of left anterior descending artery (LAD) (Figure 2B), which abruptly halted coronary flow, almost immediately resulting in cardiogenic shock. Treatment with vasopressors was promptly initiated. After a period of hemodynamic instability, she successfully underwent angioplasty of LMCA and LAD with 3 drug eluting stents (Figure 2C). She was transferred to the intensive coronary care unit (ICCU) for further monitoring and vasopressor agents could quickly be titrated down and stopped. Prompted she was transferred to cardiology ward.
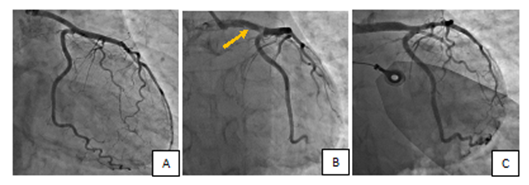
Figure 2A: Angiography shows normal coronary arteries. B. An anterograde spiral coronary dissection extending from LMCA to the distal portion of LAD is visible. C. Flow restored after stent angioplasty of LMCA and LAD.
Despite progressive improvement, at nine day of hospitalization she developed a new episode of precordial chest pain and the EKG showed >3mm ST segment elevations in the anterior leads (Figure 3).
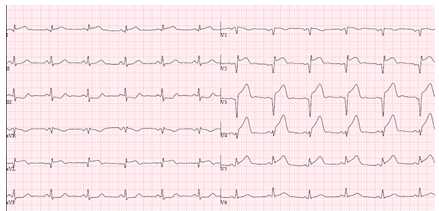
Figure 3: EKG shows sinus rhythm at a rate of 75bpm and >3mm ST segment elevations in the anterior leads.
Emergent coronary angiography revealed a proximal LAD pre-stent narrowing, probably dissection (Figure 4A). After successful LAD stent angioplasty, a circumflex artery (Cx) vasospasm resolved with intracoronary adenosine and nitroglycerine (Figure 4B/C)

Figure 4A: Coronary angiography reveals a proximal LAD pre-stent narrowing, probably dissection. B/C. After LAD stent angioplasty, a Cx vasospasm resolved with intracoronary adenosine and nitroglycerine.
Ticagrelor was switched to prasugrel an patient was again transferred to ICCU.
On further questioning, patient admitted a moderate consumption of cannabis for the last 6 months. Urine toxicology testing was positive for cannabis and negative for any other recreational drug. Subsequently the clinical course was uneventful. A pre-discharge TTE showed septal, anterior, and apical hypokinesis with reduced ejection fraction estimated at 38%. She was discharged home 15 days after admission. Post-discharge treatment included dual antiplatelet therapy (aspirin 100 mg daily and prasugrel 10mg) in combination with channel blockers, oral nitrates, and a statin.
Marijuana is the most common illicit substance used worldwide and the rate of usage is only increasing [1]. Cannabis is derived from the plant Cannabis sativa, with the main psychoactive constituent being 9- tetrahydrocannabinol (THC) [9-10]. The THC ligand has high selectivity for the Cannabinoid 1 and 2 receptors (CB1 and CB2, respectively). CB1 receptors, the primary targets of THC, are most abundant in the central nervous system, and are responsible for most CV effects via activation of the sympathetic nervous system (SNS). Those receptors are also located in some peripheral tissues, such as the heart and vascular endothelium [11-14]. CB2 receptors are found primarily in the immune tissues [15].
Different mechanisms have been proposed to explain the deleterious effects of cannabis on the heart. The most common cardiac manifestations of marijuana are a dose dependent increase in blood pressure and heart rate through cannabis-mediated activation of SNS [16-17]. Additional CV manifestations include increased myocardial oxygen demand and decreased oxygen supply due to elevation of carboxyhemoglobin [18-19]. Therefore, THC use has been associated with increased angina frequency.
While cannabis is well known to cause the effects described above, myocardial infarction (MI) or coronary vasospasm has rarely been described. In an epidemiological study to identify triggers of nonfatal MI, cannabis was shown to have a low population attributable factor of 0.8 (95% CI 0.38% to 1.67%); in comparison, cocaine use had an odds ratio of 24 [20]. Mittleman et al., in a case-crossover study found that cannabis use increases the risk of MI nearly five times within 60 min after use and confers a 1.5-3% annual risk of an acute CV event [21]. Reversible coronary vasospasm is considered the most common cause of cannabis- induced CV events [6]. While, the underlying mechanisms for this are still unclear, numerous case reports have associated THC with coronary vasospasm cardiomyopathy [22-25]. Mendizabal et al. reported that chronic marijuana use may result in autonomic nervous system dysfunction, which coupled with THC-induced irritation of the vascular endothelium could possibly explain the increased risk of vasospasm [26]. Also, the effects of cannabis induced vasospasm may be linked to THC induced mitochondrial disease in the acute coronary syndrome [3].
We present the case of a young female who, on admission, denied significant CV risk factors, besides oral birth control use. She presented symptoms and signs compatible with MI and, for that, she underwent coronarography. Initially no coronary lesions where observed, and a coronary vasospasm seemed to be the reason for the clinical picture. Unfortunately, during angiography, a coronary dissection developed. In general, iatrogenic causes of de novo dissection include catheter tip or guidewire trauma, vigorous contrast injection and angioplasty balloon overinflation [27]. Here, the procedure was performed via radial access, which requires more complex catheter manipulation than the femoral route, potentially increasing the risk of inadvertent catheter trauma. During hospitalization patient developed a new episode of MI and a second angiography was performed. After that vasospastic phenomenon became clearer and the patient confessed a regular cannabis smoking history. During hospitalization a new coronary angiography was done after a new episode of myocardial infarction and progression of the dissection in the LAD not covered by a stent was discovered. We believe that coronary vasospasm was the main responsible for the clinical picture, so the patient was medicated with nitrates and calcium channel blockers, with no pain recurrence.
Despite the symptoms here were typical, young adults with a long history of cannabis use may present with unusual clinical manifestations: recurrent episodes of nausea, vomiting, and abdominal pain. Those symptoms characterize the Cannabinoid hyperemesis syndrome, a rare medical entity observed in some long-term heavy cannabis users. While most patients usually complain of recurrent epigastric or periumbilical pain with negative investigations, the possibility of some serious cardiac event should not be neglected as cannabis seems also able to trigger coronary vasospasm in patients presenting with atypical pain or electrocardiographic changes [28].
This case illustrates the importance of recognition of vasospasm in patients taking marijuana. Myocardial infarction at a young age is unusual and drug-induced MI is gaining importance with increased use of recreational drugs. With the legalization of marijuana in certain, marijuana-related hospitalizations and ER visits are likely to increase. It is important for the clinicians to recognize the association of marijuana with CV events, namely coronary vasospasm, so a history of substance
abuse should be actively sought. Emergency physicians should consider this in the differential diagnosis of patients presenting with ischemic symptoms based on history and a urine drug screen. As this is a diagnosis of exclusion, these patients should be treated as acute coronary syndromes until proven otherwise by ischemia evaluation. However, with this case we also realize that angiography can be deleterious and cause de novo coronary dissection, a potentially fatal event if not treated immediately.
Authors declare no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
