
Research Article | DOI: https://doi.org/10.31579/2639-4162/187
1Physical Therapist NDT teacher IBITA, Course Leader and teacher on the Dutch Institute for Allied Health Sciences. Nursing Home “Waelwick” in Ewijk the Netherlands
2MSc BSc RMN Lecturer in Mental Health Nursing with Dementia Specialty. University of Cumbria, Bowerham Road, Lancaster, LA1 3JD England
*Corresponding Author: Jan Van De Rakt, Physical Therapist NDT teacher IBITA, Course Leader and teacher on the Dutch Institute for Allied Health Sciences. Nursing Home “Waelwick” in Ewijk the Netherlands.
Citation: Jan Van De Rakt, Steve M. Grunwald, (2024), Can Disturbed Perception Be Improved Through Task-Specific Resistance Treatment at A Stroke Patient? J. General Medicine and Clinical Practice, 7(11); DOI:10.31579/2639-4162/187
Copyright: © 2024, Jan Van De Rakt. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 May 2024 | Accepted: 10 June 2024 | Published: 18 June 2024
Keywords: stroke; perception; task specific training; muscles- input-perception
Aid:
We know that the perception of people after an stroke is disturbed and that this give this people an extra problem to handle. We know further that when the tone is high and the selectivity is poor than the disturbances of the perception is often extreme. That give by some patients an fear that is almost not to understand.
Materials and Methods:
The purpose from this study is to try an intervention to improve the perception. The hypothesis that we try to prove the perception of his body sec but also in the environment was, that in the total program of the rehabilitation we explicit give more task-specific resistance treatment for the affected leg in stand phase to get through the better working of the muscle spindles and better coordination and through that also an better perception of his body sec but also of his body in his environment.
Results;
His power an coordination was clearly translate in better and faster walking in the exercise department and there were with adaptation some improvements in the ADL (Activities of Daily Living) at his home but the test of the perception of his body stay almost the same
Conclusion;
Improvements were absolute there but they were visible in the walking speed and walking with different aid. But the test that gives us an picture of the perception gave no great improvement. The passive test stay the same but when the muscle spindles were used there was an improvement and what was clear is that this cost an great amount of time over an long period and when the training stop the result were decreasing. Authorship credit: “Criteria authorship scientific article” has been used “Equal Contribution” (EC). Citation:
jan@vanderakt.nl
Impairment of the perception, the translation of input (from tactile, vibration, two-point discrimination, proprioceptive input etc. [1]. is the system that the literature is called the somatosensory afferent system. By person after an stroke is this system intact all away till the brain, but there are signals [2] that this system will adapt in time and his frequency of firing will decrease,
The biggest problem by patients after a stroke is assimilation of all input in the damage brain and the possibilities that this brain has to instructed the efferent system. Kluger [3] has investigated this and he found, that there is an delay in the transport and assimilation of stimuli and that can lead to less perception or as he called it “less perceptual awareness “. And his conclusion is therefore that through this the possibilities are obvious lesser. A small group of patients after an stroke, in the literature is not to find how much, had this problem such an problem that they never will build up an reasonable walking pattern. Walking stays for them a tremendous problem that so much asked that this people will choose for the wheelchair and walking rather try to avoided in the participation though the day. [4]
Case Gentlemen T.A.
A gentleman of now 55 years, who has 10 years ago had an severe stroke. Beside the loss of perception on his affected side, he has also a severe hemianopia, that makes his visual control extra difficult. Still, he lives independent, but much he doing sitting at home in a wheelchair, certainly because he was fallen at home and had broken his hip on the affected side. He was capable to walk with a hand-stick, behind a high chair but on the moment that someone asked him something or when he heart somethings strange than he stop withy walking. (Stop Walking When Talking - S.W.W. T. [5] When he was walking in the therapy with no aid or with an Nordic walking stick, often was than there the moment that stand still and dare not walk further and cry for help (freezing). He stays in that standing position and could only further when some give him an hand-on facilitation and he was often for an hour in panic, In the last year this behavior was increase and he was not able at home to pick something and walk with it, only walking with his stick was at home possible but that hasn’t no value because he couldn’t take something with him, therefore was the function in his affected arm/hand to bad.
Motricity Index (M.I.): Arm = 28: in shoulder14 and elbow 14 and hand 0.M.I.
Leg = 28 Hip 14, knee 14 en foot 0.[6]
His main question was:
Walk without in stick at home because otherwise this exercising has no value for me!”
This question means, that the perception must improve to get that degree of independent walking at his home. This must also be automatic so that he can focus on a task as carrying something through his house. As this automatism cannot achieve than he needs so many attentions for his walking that he is never capable to carry something through his house, certainly not a full glass!
Search in the literature.
From the past two books were know by us, that were books that pointed on the possibilities that perception/ sensorics /preprocess was an item that can improve through treatment The approach Rood [7] with skin stimulation direct above the muscle that must be stimulated was done by dorsal flexors of the foot and knee extensor muscles. This gave more feeling at the beginning but was often after two steps extinguish. The treatment according Yekutiel [8] was pointed on the treatment of the arm but the stimulation of the two discrimination – feeling can be very important for the foot. Now he feels his foot at the ground but not how and that he must control visual and that was an great problem. He was not capable to feel or he stand correctly on his foot and that he doesn’t fall backward when he lifts and place his not-affected foot. All this treatment has no value because his attention on the discrimination- possibilities of the foot was possible in sit but in stand wasn’t it possible that he makes attention free for this because he has it elsewhere needed. Search in PubMed gave as a result of 7 articles [,3,9,10,11,12,14,15] including 3 articles [9,11,12] that pointed on the “pusher-syndrome. That this is this case play an role was clear but there was no clear answer “how to stimulated the perception “. There were articles that focus on the Why and How important perception is [3,10] and only one article [14] try an treatment. This was done by giving electric stimuli on the fingers and that is seem possible that the discrimination- feeling was improved and that hold about 4 weeks after the treatment. Application of this electro therapy (TENS 50 Hrz-120µs) was a success in sit but after a few meters walking this feeling was gone.
Only Sato [15] that capable to show that on nerve level a brain level something change in the senso-motoric cortex as someone moves in water. This effect is only there when that part of the body was fully submerged and as that person moves. Well has Patten [18], but also in the guidelines of the Royal Dutch Society Physiotherapy [16] (K.N.G.F.), and [19/20] pointed out that muscle strengthening by stroke patients has an positive effect certainly in combination with task specific exercising, but to give an muscle- strengthening to get an improvement of the perception, seem to us an bridge to far. In his article give Martin Moons [1,13] clear how important it is that the muscle spindles are for the preprocess and the correct tension can change the perception. This is confirmed by Henri Kiers [17] in thesis about patient with back pain problems. In this thesis he proves that balance by back pain patient can be disturbed through this person let stand on an unstable platform and vibrated the low spine muscles. Vibration on the muscle is a method to influence the muscle spindles negative. Patients stand on a stable platform than the vibration on the back had no effect, but was the vibration on the calf muscles was the greatest disruption. On an unstable platform was the vibration of the back muscles the greatest disturbance by back pain patients. Therefore, less propriocepsis from the muscle’s spindles had an influence on the holding of the balance, certainly when the underground was unstable. Back complaints have a negative influence on the propriocepsis of the back muscle and that give an perception than was decreased. Patients after a stroke will have certainly an interruption of the function of the muscles spindles because the tone is often not normal, but would it be possible that task-specific training has an effect on it as by people with back pain? Task specific strengthening gave by an number of stroke patients an coordination improvement [18] Therefore could it be possible that the influence of the muscles spindles can improve the perception. But it must be task specific and that asked for an analysis of the walking performance and especially there where the biggest problem lies. Top trainers focus on that task-specific by injuries must almost perfect fit in the task- specific and that training of isolated muscles give an very difficult transfers to the task specific movement.[21]
Investigation question.
Is it possibility that task-specific muscle strengthening can improve the perception of the leg and had that as result that he can better walk and can we generate an form of automatic walking?
The participation level when he is walking must be so change so much, that he can use this on participation level the whole day at least at his own home!
To investigated this, we must know what during the walking performance the most difficult moment is and which muscles are at that moment essential. Through a strengthening of the group of this muscles or muscles pattern, must there create a grow of the feedback and that must create an greater feeling of security and more perception.
Analysis of the walking-pattern.
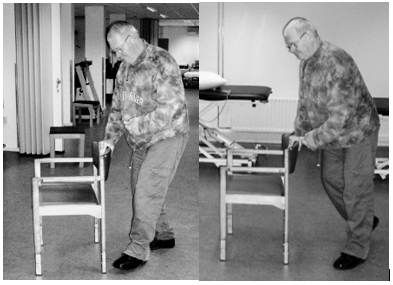
Photo 1 Photo 2
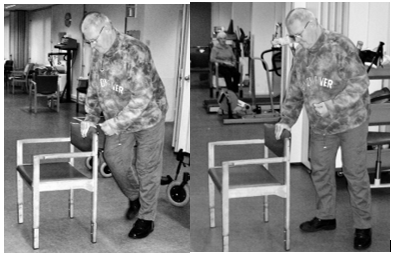
Photo 3 Photo 4
Analysis of the most difficult moment.
Photo 1.
Give a picture on the end of the swing phase en the start of the stand phase (“Heel strike) of the affected leg. There is on this way no real heel strike, because the tone in the plantar flexors in the leg is than so high that the foot is placed flat on the whole foot with almost no load. Further-one is the ankle mobility restricted to maximum of 90 ˢ. The ankle has an double peroneus string (EVO) with an T- aid to hold the ankle in the right position with not too much eversion. The foot is placed with a blow. Attempts to decrease the amount of striker foot are all failed. A test treatment with lidocaine gave a total loss of the perception and after that he couldn’t walk. Casting was for him no option because he couldn’t stay at home.
Photo 2
Loading response. The time between photo 1 -2 to 3 is long. This goes very slow and asked fora n great amount of attention
Photo 3 mid-stance.
Also, this moment to get the weight on his affected foot and make the not-affected foot ready for the swing phase cost also much time. He stays for some seconds complete still and his amount of support on the chair rest is great.
This is the moment that is goes wrong most of the time. When he isn’t certain that all is right, he will stop and in the best case he goes back but otherwise he will than cry for help.
Photo 4.
He stands again on his not-affected led and we see that the movement over his affected hip isn’t complete because through the restriction in the foot and in the hip, he must make and rotation away from his affected hip. A push-off of his affected leg isn’t present.
The moment with the greatest problems and with his greatest attention is the moment that he starts with placing load on his affected leg. Then is it important that he isn’t stand still too long because than the extinction take place and goes all wrong.
With the chair support in front of him he can solved this through take a huge amount of support on the chair. And through the position of the chair in front of him is a great amount of his body fast in front of the affected foot/leg. But when he walks with a stick or even without an aid than must there be an concentric contraction in his gluteal muscle to get an movement to the front, to come over or better along his affected foot. That contraction must he “experience” through the muscles spindles and his brain must register this – perception.
“Normal action “after the heel strike goes the movement as follow;
Prof. J. Buurke [22] in his thesis about walking that the heel strike is the moment for the great gluteal muscle to act. This more than enough power to “push” us over the hip. But by the patient in this casus is no heel strike present and he must build up this tension /contraction when he stands on his affected leg and that will happen when he lift his not-affected leg. But this contraction will not be concentric but a reaction on the elongation of the muscle. And the moment is with his body behind affected foot and will not transfer the body over the foot and hip. When we look to the diagonal principle [23,24,25]is the concentric action of the gluteal muscle an important part of the back diagonal but this muscle has mostly fast fiber structure and that is by people after a stroke a muscle that fast decrease or changes in a slow muscle. To get an action in this muscle or to activated this muscle the patient will use the whole diagonal, especially the part on the not-affected side and that is possible by using a stick to push away. Still, this asked for a concentric action also when this isn’t possible, therefore will the patient be lengthening the muscle. Lieber [26] write that this lengthening can give an action on spinal level, this is still no eccentric contraction, because than there is an action within the cortical area. This is only a stretch reaction on the muscle spindles and through the spine segment back to the muscle.
Looking at photo 2 and 3 and comparing this two with the other two, than is the amount of support on the backside of the chair gigantic. And his upper trunk moves almost over this backside. That means that the amount of pressure on his not-affected arm is great and that the back diagonal starts here and goes to the affected leg. There is a contraction in the gluteal because between photo 2 and 3 there is no more flexion in his hip. Still is there a change that the adductor muscle created the extension because the diagonal is maybe not ended in the “heart” of the hip.
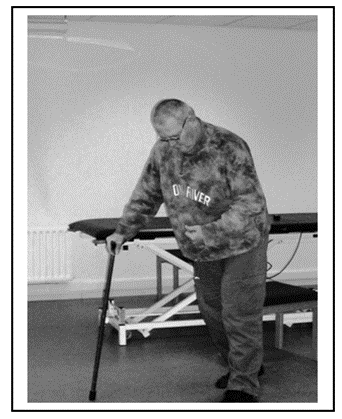
Photo 5: Look when he walks with a normal cane and compare it with walking behind a chair or special rollator frame. The placing of the cane is far in front of him and far lateral also. Still, he places a great amount of support to activated the back diagonal from the not-affected arm/upper trunk to the affected leg. Even the index finger pointing to floor must help to activated the extension power of his affected leg.
This moment was often very important! when he “feel” that his affected leg give an answer, he walks further but when that feeling wasn’t there than he freezes.
At the moment that he freezes no info came from his affected leg and he must have someone else to get him walk again. Therefore, he must “feel” his affected leg!!
Hypothese
Foto 5
Hypothesis
Would it be possible through Task Specific Resistance Therapy increase the concentric power of the gluteal muscles and would that have an effect on the coordination and also on the perception of the affected hip muscle
But first we must know what his perception possibilities are because than we can search for an improvement.
Test for Perception.
Test for perception is present but often debating about their validity.
Therefore, have we chosen for an combination of several test.
1. The propriocepsis and movement- feeling but almost never in the task itself. That means that we have an image of the perception but we need to create an translation to the task. The propriocepsis and movement –feeling was tested through the “Lage –und bewegungssinn” writing by Marks [27]and in the book “Assessment in der Neurorehabilitation” [28]) has the validity be studied:
2. “When the results are the number of degrees that the person has failed than this test is reasonable reliable “! Failures of more than 11° by great joint, and more than 5° by the knee. For the foot is this not sure but we hold more than 5 ° on. This test must be done in lying position and that is disadvantage because it isn’t in the task. The 10-meter walking test [29] makes clear what the possibilities of the patient are. Walking under supervision asked for a speed of 0,27 m/s, independent walking inside asked for a speed of 0.53 M/S and walking around the house asked more 0.70 m/s and normal walking is 1,17m/s, according Koolstra [29]. But it gives a clue what we need for an speed to stay independent with an walking capacity that is “automatic” more or less, but with an base of perception in it.
Stop Walking When Talking (S.W.W.T.) –test. This test we could use to test how far he was able to walk automatic”.
Before the task- specific training, the results of the 3 test on propriocepsis test ( A. mirror technique, B. movement feeling without active tension and C. with active tension were:
Test A.
Mirroring.
Knee 65 degree wrong – 3 times after each other tested (flexion – Extension movement)
Hip 50 degree wrong - 3 times after each other tested (flexion –Extension movement)
Exorotation from neutral position 15-20 degree wrong 3 times after each other tested.
Test B
Movement –feeling without active tension/movement.
Knee 40 degree wrong - 3 times after each other tested (Flexion-Extension)
Hip 50 degree wrong- 3 times after each other tested (Flexion –extension)
Exorotation from neutral position 15 degree wrong – 3 times after each other tested.
Test C
Movement –feeling with active movement.
Knee 20 degree wrong - 3 times after each other tested. (Flexion- Extension)
Hip 20 degree wrong -3 times after each other tested. (Flexion –extension)
Exorotation from neutral position 15 degree wrong – 3 times after each other tested.
Clear that in the case there is a great perception problem and he gave the best performance when he was able to move together with the investigator (test C). But this are test in lying or sitting position and impossible to test in stand but we have no wan indication what her “feel in his brain “.
10meter walking test
With different walking aids to achieve that the training was possible with much variation because we search for the best translation of the walking at his home later on.
Walking- test was done 3 times and the best [performance was recorded.
In this test, we choose to start at the highest level of speed he can perform, walking through the finish-line, this according Koolstra – on page 78 [29].
| 10 meter walking test | Time | M/S | M/m. | Km/h |
| 1. Walking- test behind high chair (photo 1) | 40 sec | 0.25 | 15 | 0.90 |
| 2. Walking -test behind special rollator frame (Photo 6) | 42 sec | 0.23 | 14.28 | 0.85 |
| 3. Walking -test with normal cane (photo 5) | 45 sec | 0.22 | 13.33 | 0.8 |
| 4. Walking-test with Nordic Walking stick. | Not possible | |||
| 5. Walking-test behind chair and with another task. S.W.W.T. | Not possible |
M/S = Meter per second. M/m = Meter per minute. Km/H= kilometers per hour.
Table 1: Impression for the start of the extra task-specific resistance training.
Photo 6: His walking attitude don’t change much. Every time is this moment the most difficult moment when he searches for the optimal situation that he feels that he can manage the load on his affected leg and can lift his not-affected leg to the front. A high amount of visual control, attention and an bended trunk to stretch the extensors of the hip. He cannot with this rollator frame go so far over the support point as with the chair and that is in influence of the rollator -form/wheels. His speed (table 1) is lower than the supervision speed of Koolstra (0.23 M/S - Koolstra 0,27 m/s.)
The base treatment was 3 times a week:
The extra part of the training was:
Ad 1. To get an good power training (strength × speed) for the gluteal muscle group in his task, thus when the movement over the affected hip take place and the affected leg is in the stand phase, wasn’t easy.
There were some problems that had to eliminated:
Translated this to the practice:

Photo 7: Task- Specific resistance training.
Resistance is given against the not-affected leg. This resistance is given through the whole swing movement when this possible. From the start when the not-affected leg stands behind the affected leg till the end at the start of the heel-strike of the not-affected leg. This to get a contraction in the extensor muscle of the affected hip in the stand-phase movement over the affected hip.
Problems that there were to start this program.
At the start the movement that he makes, was especially in the upper trunk. This he did, to get tension on the muscle Gluteus Maximum trough an elongation of the muscle. This would mean that this contraction was a contraction on spinal level and therefore will give no reaction in the brain and no perception improvement. Therefore, we must search how to inhibit the trunk elongation and more important how we can create an contraction in the hip extensors that has concentric elements. Because this element is supra-spinal and would have an effect in the brain. This was possible to do the movement without resistance but with a good stabilization of the affected leg and his trunk. After that we give an little resistance against the swing phase of the not-affected leg and now it was certain that the hip extensors gave an concentric contraction we could increase the resistance an little in the beginning. Often this give a cramp in the beginning and was it not possible to get the amount of rehearsal.
In the measurements can be find back as we look to the walking speed test. These measurements of the walking speed were done 4 times;
The second extra training was:
Statiek –Training. [30,31] The principle of the statiek training is that we give little pressure at the pelvis or at shoulder height to test the reaction of this person on that pressure. This pressure is given to the back, but also a pull to the front. Further can this also done on left and right side to assess or the person is capable immediately to react on that pressure. Second part is the reaction as this pressure is suddenly withdrawn. In this casus was the patient not capable to create a reaction as there is given pressure on the front, but also was not capable to given the right reaction on the not-affected side but there was a little reaction. The reaction when the pressure was gone was negative. Was this test done on shoulder height on the front there was almost no reaction. The pull on the back side gave an trunk inclination and at the end of the flexion was some resistance that means that he wasn’t capable to give resistance against this pull and must the gluteal muscle give an stretch to get an reaction. Never was he capable to get an situation that he brace the fall to the front by toe standing. After the training was this part still very difficult but there was at the end an reaction on the affected side and there was at the end an better reaction of the hip-extensor and some better balance. One leg standing G [RAMPS 32] at the beginning was standing on his affected leg impossible when there was no support on the not-affected side in the beginning an stable table, latter on an chair. And he must be first lifting his not- affected leg against resistance with support of an chair and then he could do an one leg standing at the end of the training period of 20 sec. with eyes always open.
| 10 meter Walking - test | Time | M/S | M/m | Km/h |
| 1.Walking test behind chair. | 38 sec | 0.26 | 15.78 | 0.94 |
| 2.Walking test behind special rollator frame. | 40 sec | 0.25 | 15 | 0.9 |
| 3. walking test with normal cane. | 42 sec | 0.23 | 14.28 | 0.85 |
| 4. Walking test with Nordic Walking Stick. | 60 sec | 0.16 | 10 | 0.6 |
| 5. Walking test with chair and extra task. S.W.W.T. | Not possible |
Table 2 -Task Specific Muscle Resistance Training and statiek after 10 weeks.
| 10 meter Walking test | Time | M/S | M/m | Km/h |
| 1. Walking test behind a chair. | 32 sec | 0.31 | 18.75 | 1.12 |
| 2. Walking test behind special rollator frame. | 34 sec | 0.29 | 17.64 | 1.05 |
| 3. Walking test with normal cane. | 36 sec | 0.27 | 16.66 | 1 |
| 4. Walking test with Nordic walking Stick. | 40 sec | 0.25 | 15 | 0.90 |
| 5. Walking test with chair and extra task. S.W.W.T. | Not Possible |
Table 3-Task Specific Muscle Resistance Training and statiek after 20 weeks.
| 10 meter Walking test | Time | M/S | M/m | Km/h |
| 1. Walking test behind chair. | 17 sec | 0.59 | 35,3 | 2.1 |
| 2. Walking test behind special rollator frame. | 19 | 0.53 | 31.6 | 1.9 |
| 3. Walking test with normal cane. | 20 sec | 0.5 | 30 | 1.8 |
| 4a. Walking test with Nordic walking Stick. | 21 sec | 0.48 | 28.6 | 1.7 |
| 4b. Walking test without a cane. | 3 meter | |||
| 5. Walking test with chair en extra task. S.W.W.T. | Not possible * |
Table 4- Task Specific Muscle Resistance Training and statiek after 30 weeks.
* in the three test-sessions, once he was able to walk through an make math. His time was 40 sec. over the 10-meter walking test.
Smallest Detectable Difference (SDD) for the 10-meter walking test is -- 0.16 m/s.
Improvement in the time.
| Start | 10 weeks | 20 weeks | 30 weeks | Difference Total | Difference 20-30 w | |
| Green chair | 0,25 | 0,26 | 0.31 | 0.59 | 0,34 ** | 0.28** |
| Special rollator frame | 0,23 | 0,25 | 0.29 | 0.53 | 0,3 ** | 0,24 ** |
| Normal cane | 0,22 | 0,23 | 0.27 | 0.5 | 0, 28 ** | 0.23** |
| Nordic Walking | - | 0,16 | 0.25 | 0.48 | 0,32 ** | 0,23 ** |
| Without | - | - | - | - | - | |
| Green chair and SWWT | - | - | - | - | - |
** all these values were above the SDD norm.
Perception developmental?
After the 10-20-30 weeks we have also done the perception tests and look at his attitude changes.
Participation level after 30 weeks;
There was a significant improvement in faster walking with an lot of aids.
In his apartment he was also faster with a normal cane and along the wall and the 3 meters without he uses in the kitchen.
Walking in the corridor was better but especially faster.
But open space, such as the mid of the therapeutic ward was still difficult.
There was therefore no generalization but a small participation improvement but only there were he had exercised and therefore also in his apartment.
After 10 weeks.
Test A Mirroring
Test B Movement feeling without active tension/movement.
Test C Movement feeling with active movement, own contribution.
Test A and B no change.
Test C there seem to be a difference, but that wasn’t expressing in degrees.
This was around the 20° for flexion/extension hip and knee and 15° exorotation in the hip.
After 20 weeks
Test A Mirroring
Test B Movement feeling without movement/tension.
Test C Movement feeling with active movement and own contribution.
Test A en B no change.
Test C again it looks like an progression but not measurable in degrees. Maybe that he knows the measurements now?
After 30 weeks.
Test A Mirroring
Test B Movement feeling without active tension/movement.
Test C Movement feeling with active movement and own contribution.
Test A and B they were different as 10 weeks before but the measurement was almost the same.
Test C Here was the change measurable: In the hip 5ᵒ less, now around the 15 ᵒ. Also, the knee 5 ᵒ lesser. The extension stays around the 20°for hip and knee.
The exorotation was still around the 15 ᵒ.
Attitude.
Increasing of the tone in the buttock muscle can also have an effect on the attitude, because the flexion of the trunk isn’t necessary anymore.

Photo 8 Photo 9
Photo 8: Walking with Nordic Walking Stick after 10 weeks. The horizontal line is equal with the radiator and then the inclination of the trunk. This angle is 25 ᵒ.
Photo 9
Walking after 30 weeks and the horizontal line is now fixed on the wall structure.
The angle is now 14 ᵒ.
That is a significant progression of 13ᵒ.
A significant improvement of the walking speed on the same place in the therapeutic ward of a nursing home but ……elsewhere? But the improvement of the perception through more coordination and power is a question that remain open, there is no answer from this investigation. But one conclusion can be done: there are signs that the last 10 weeks had the most changes and maybe we must do this over a much longer period. Also had his attitude improved and that is also a combination of muscle tone and perception. We also observed that he couldn’t keep this level on his own. In a holiday period he decreases with his speed on the level between 10 and 20 weeks. Are his participation possibilities increased? His stair raising is improved and he walks between the stairs through without a support. In the kitchen he works in standing position without a cane and is out his wheelchair what very difficult was in that small area. The remaining part of the house he walks along the wall and with a cane, but often with the cane off the ground. Again, the same feeling as with the walking speed, we stop too early. Further investigation by person with this degree of perception loss, this approach must do minimal 60 weeks with increasing difficulties and resistance.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
