
Review Article | DOI: https://doi.org/10.31579/2693-2156/036
* Critical Care Unit, Al-Rodah Central Hospital, Damietta Health Affairs, Egyptian Ministry of Health (MOH), Damietta, Egypt.
*Corresponding Author: Yasser Mohammed Hassanain Elsayed, Critical Care Unit, Al-Rodah Central Hospital, Damietta Health Affairs, Egyptian Ministry of Health (MOH), Damietta, Egypt.
Citation: Elsayed Y M H, (2022). Camel-Hump T-Wave, Tee-Pee Sign, and Wavy Triple Sign (Yasser’s Sign) with Hypocalcemia and Hyperkalemia in Covid-19 Pneumonia with Lacunar Infarction. J Thoracic Disease and Cardiothoracic Surgery, 3(1); DOI:10.31579/2693-2156/036
Copyright: © 2022 Yasser Mohammed Hassanain Elsayed, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 December 2021 | Accepted: 27 December 2021 | Published: 07 January 2022
Keywords: COVID-19; camel-hump T-wave; tee-pee sign; wavy triple sign (yasser’s sign); hypocalcemia; hyperkalemia; lacunar infarction; cerebrovascular stroke
Rationale: A novel COVID-19 is a multi-systemic critical worldwide pandemic infection. Certainly, associated multiple electrolytes imbalance in COVID-19 pneumonia is a remarkable decisive event. Camel-hump T-wave, Tee-Pee sign, and Wavy triple sign (Yasser’s sign)are novel highly significant descriptive electrocardiographic signs that are seen in calcium and potassium disturbance. There is an established and strong relationship between and electrocardiographic abnormalities and electrolytes imbalance. COVID-19 pneumonia and cerebrovascular stroke are commonly seen in a patient with Coronavirus infection.
Patient concerns: A 69-year-old married worker Egyptian male patient was presented to the emergency department with COVID-19 pneumonia and cerebrovascular stroke.
Diagnosis: COVID-19 pneumonia with lacunar infarction, hypocalcemia, and hyperkalemia.
Interventions: Chest CT scan, brain CT scan, electrocardiography, oxygenation, and echocardiography.
Outcomes: Initial bad and deterioration outcome but, the dramatic outcome had happened after later management.
Lessons: The understanding of electrocardiographic signs regarding metabolic disorders such as electrolytes imbalance and other associated systemic diseases is very important. Elderly male sex, heavy smoker, COVID-19 pneumonia, cerebrovascular stroke, chronic renal impairment, ischemic heart disease, hypokalemia, hypocalcemia, and hypernatremia represent bad prognostic points and is indicating a high-risk condition.
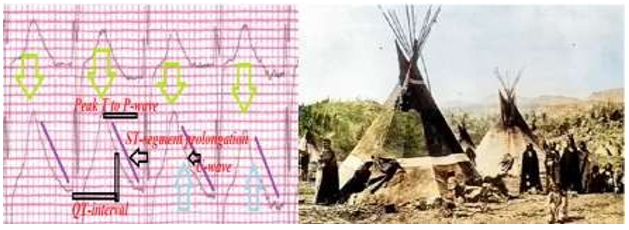
Generally, in medical diseases, the clinical response is commonly parallel to laboratory and electrocardiographic improvement. A direct relationship between clinical status, ECG, and laboratory workup is essential [1]. Early studies had recorded different electrolyte disturbances at admitted patients with severe COVID-19 infection. As electrolyte imbalance mainly affects the impact of patient care rather than the pathophysiology of COVID-19 [2]. Periodic measuring of electrolytes after the initial presentation during hospitalization is a target to timely establish and appropriate corrective management [2], The relationship between electrolytes disturbance and coronavirus disease 2019 (COVID-19) in patients of the emergency department (ED) is still vague [3]. The role of the ECG in the assessment and management of acutely unwell patients has long since extended beyond the evaluation of chest pain [4]. Johri et al (2009) reported a case of a combination of hyperkalemia and hypocalcemia resulting in pre-cordial QRS-complex with peaked T-wave, prominent U-wave, and prolongation of the descending limb of the T-wave. This resulted in the T- wave overlapping the U wave and they called it the “Tee-Pee Sign” because the shape of the QRS complexes resembled the traditional shape of native American Indians dwelling (Figure 1). The combination of prolongation of both the ST segment and descending limb of the T- wave resulted in pseudo-prolongation of the QT interval [5]. Camel- hump T-wave is not specific for electrolyte imbalance. The presence of multiple severe electrolyte abnormalities is the cause for this very dramatic camel-hump T-wave, formed by fusion of the T-wave and Giant U-wave [4]. Multiple electrolyte imbalances and have observed dramatic ECG changes of camel-hump T waves and the “Tee-Pee sign”. A combination of electrolyte imbalance has not previously been reported and this is the most dramatic example of camel hump T-wave [5]. Wavy triple an electrocardiographic sign (Yasser’s sign) is a new specific diagnostic sign seen in 97.3% of the cases of hypocalcemia. Wavy triple an electrocardiographic sign can be used as a therapeutic guide in the cases of hypocalcemia [6]. Coronavirus disease2019 (COVID-19) evolved quickly into a global pandemic with myriad systemic complications, including stroke.COVID-19 is an independent risk factor for stroke in hospitalized patients and mortality, and stroke presentations are frequently atypical [7].
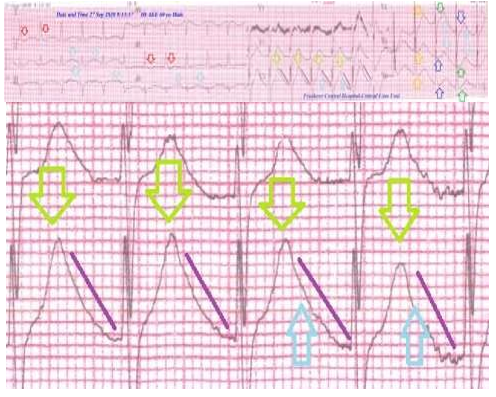
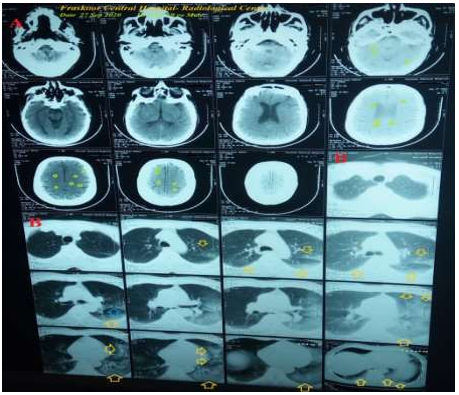
A 69-year-old worker, married male, Egyptian, heavy smoker patient was presented to the emergency department (ED) with tachypnea, left- side heaviness, generalized body aches, and palpitations. Fatigue, dry cough, anorexia, and loss of smell were the associated symptoms. There is a recent contact with a confirmed case of COVID-19 pneumonia. He was presented to the ED within 5 days of the above symptoms. He gives a history of chronic renal impairment. He is smoking about 20 cigarettes for17 years. The patient denieda history of cardiovascular diseases, the same attack, drugs, or any other special habits. Informed consent was taken. Upon general physical examination; generally, the patient was tachypneic, distressed, with a regular pulse rate of VR; 120 bpm, blood pressure (BP) of 150/90 mmHg, respiratory rate of 27 bpm, the temperature of 37.8 °C, and pulse oximeter of oxygen (O2) saturation of 87%. There is left-side hemiparesis with GCS; 12. Tests for latent tetany were elicited. Initially, the patient was treated with O2 inhalation by O2 cylinder (100%, by nasal cannula, 5L/min). The patient was maintained treated with cefotaxime; (1000 mg IV every 8 hours), azithromycin (500 mg PO single daily dose), oseltamivir (75 mg PO twice daily only for 5 days), and paracetamol (500 mg IV every 8 hours as needed). SC enoxaparin 80 mg twice daily), aspirin tablet (75 mg, once daily), clopidogrel tablet (75 mg, once daily), and hydrocortisone sodium succinate (100 mg IV every 12 hours) were added. The patient was daily monitored for temperature, pulse, blood pressure, and O2 saturation. The patient was managed in the ICU with COVID-19pneumonia, ischemic heart disease, lacunar infarction, hyperkalemia, hypocalcemia, and hypernatremia. The initial ECG was done on the ICU admission showing sinus tachycardia VR; 118, ST-segment depression in both high lateral leads (I and, aVL), Camel-hump T-wave (II, III, aVF, and V3-5), Tee-Pee sign with ST-segment prolongation (V3), and Wavy triple sign Yasser’s sign of hypocalcemia (V4-6 leads (Figure 2). The first brain CT without contrast was done during the day of hospital admission showing lacunar infarction (Figure 3A). The first chest CT without contrast was done during the day of hospital admission showing destructive left ground-glass opacities(Figure 3B).
Currently, the patient was admitted to the critical care unit with COVID-19 pneumonia, cerebrovascular stroke, chronic renal impairment, and ischemic heart disease. The initial complete blood count (CBC); Hb was 10.9 g/dl, RBCs; 4.1*103/mm3, WBCs; 19*103/mm3 (Neutrophils; 87.5 %, Lymphocytes: 8.3%, Monocytes; 4.2%, Eosinophils; 0% and Basophils 0%), Platelets; 174*103/mm3. S. Ferritin was high; 494 ng/ml. D-dimer was high (0.916 ng/ml). CRP was high (97 g/dl). LDH was high (538 U/L). SGPT was normal (41 U/L), SGOT was normal (36 U/L). Serum creatinine was high (4.7 mg/dl) and blood urea was high (154 mg/dl). RBS was normal (188 mg/dl). Plasma sodium showed hypernatremia (152 mmol/L). Serum potassium showed hyperkalemia (5.8 mmol/L). Ionized calcium was low 0.62 mmol/L). The troponin test was negative (0.03 U/L). CK-MB was normal (11 U/L). The echocardiography was done on the presentation showing mild grade I, diastolic dysfunction with an EF of 63%. Two calcium gluconate ampoules (10 ml 10% over IV over 20 minutes) were given as an emergency dose. Maintenance therapy with IVI calcium gluconate ampoules (10% with the rate; 0.5 mg/kg/hour over IV over 6 hours) was infused. Act rapid insulin was added in 500 ml of 10 percentage dextrose 5% IV infusion. Periodic inhalation nebulizer sets with salbutamol drops were given. COVID-19 pneumonia, ischemic heart disease, lacunar infarction, hyperkalemia, hypocalcemia, and hypernatremia was the most probable diagnosis. The patient was discharged within 7 days of hospital admission nearly, after clinical, electrocardiogram, and workup improvement. The patient was continued on aspirin tablet (75 mg, OD) for three months, long standing nitroglycerine oral capsules (2.5 mg BID), and calcium with vitamin D oral preparations (OD) for 2 weeks with follow-up. Further cardiac, renal, neurological, and chest follow-up was advised.
Overview:
A 69-year-old married worker Egyptian male patient was presented to the emergency department with COVID-19 pneumonia, ischemic heart disease, lacunar infarction, hyperkalemia, hypocalcemia, and hypernatremia. The primary objective for my case study was the presence of a patient who presented with COVID-19 pneumonia, ischemic heart disease, lacunar infarction, hyperkalemia, hypocalcemia, and hypernatremia in the ICU. The secondary objective for my case study was the question of; how did you manage the case at home? There was a history of contact with a confirmed COVID-19 case. The presence of confirmed COVID-19case, left-side ground-glass consolidation, and laboratory COVID-19 suspicion on top of clinical COVID-19 presentation will strengthen the COVID-19 diagnosis. Interestingly, chronic renal impairment with tachypnea due to COVID-19plays an essential role in the present hyperkalemia and hypocalcemia. Elderly male sex, heavy smoker,COVID-19 pneumonia, cerebrovascular stroke, chronic renal impairment, ischemic heart disease, hypokalemia, hypocalcemia, and hypernatremia are risk factors.
QTc prolongation was the most probable electrocardiographic differential diagnosis for the current case study. but the QT interval in hypocalcemia rarely exceeds 140% of the normal5. I can’t compare the current case with similar conditions. There are no similar or known cases with the same management for near comparison. The only limitation of the current study was the unavailability of serial workup.
There are no conflicts of interest.
I wish to thank the team nurses of the critical care unit in Fraskour Central Hospital who make extra-ECG copies for helping me. I want to thanks my wife to save time and improving the conditions for supporting me.
COVID-19: Coronavirus disease 2019
ECG: Electrocardiogram
ED: Emergency department
ICU: Intensive care unit
O2: Oxygen
SGOT: Serum glutamic-oxaloacetic transaminase
SGPT: Serum glutamic-pyruvic transaminase
VR: Ventricular rate
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
