
Case Report | DOI: https://doi.org/10.31579/2690-1919/408
1 Bachelor's Degree in Podiatry from the University of Seville. Official Master's Degree in Foot Surgery from the Catholic University of Murcia. Honorary Research Assistant in the Department of Podiatry at the University of Seville. Address: C/ Avicena s/n, Seville, 41007. Lead author. Responsible for drafting the clinical case and sample collection. https://orcid.org/0000-0001-9956-6263
2 Bachelor's Degree in Podiatry from the University of Seville. Official Master's Degree in New Care Trends in Health Sciences from the University of Seville. Honorary Research Assistant in the Department of Podiatry at the University of Seville. Responsible for drafting the clinical. https://orcid.org/0000-0002-1985-4968
3 Contracted Professor Doctor, in the Department of Podiatry at the University of Seville. Article reviewer. https://orcid.org/0009-0008-6181-870X.
*Corresponding Author: Rayo-Pérez Ana María, Bachelor's Degree in Podiatry from the University of Seville. Official Master's Degree in Foot Surgery from the Catholic University of Murcia. Honorary Research Assistant in the Department of Podiatry at the University of Seville. Ad
Citation: Rayo-Pérez Ana María, Rodríguez-Castillo Francisco Javier, Raquel Garcia de la Peña, (2024), Calcaneal bone edema. A case of series, J Clinical Research and Reports, 16(5); DOI:10.31579/2690-1919/408
Copyright: © 2024, Rayo-Pérez Ana María. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 September 2024 | Accepted: 18 September 2024 | Published: 16 October 2024
Keywords: bone edema; calcaneus; heel pain; chronic pain; plantar fascitis; neuropathy
bone edema or bone edema is an uncommon pathology in podiatric practice. However, there are some cases we can detect within it. This bone alteration results from trauma, degenerative lesions, or metabolic processes, with the first being the most common cause. It is characterized by acute pain in the heel area, which gradually becomes more generalized, as well as redness and swelling of the area. In the initial stages, the use of NSAIDs or analgesics is recommended, and in more advanced stages, drainage of the area. This study is aa prospective observational study analyzing 20 subjects with calcaneal bone edema. Various surveys such as AOFAS, SF-36, and VAS are conducted to fully analyze the condition and its evolution after 3 months and 6 months post-treatment. Following the intervention, there is a notable improvement in the patients' quality of life, as well as a significant reduction in pain. In conclusions calcaneal bone edema is an underdiagnosed pathology mainly due to its lack of recognition and low prevalence. It is essential to know the differential diagnosis with other heel pains to comprehensively address this condition.
Heel pain, known as talalgia, affects 14% of the population at some point in their lives. It is a common clinical condition that typically resolves spontaneously within 10 to 12 months from the onset. However, in the remaining 10% of cases, it progresses into a chronic pain syndrome, characterized by a complex array of conditions such as recalcitrant fasciopathy, Baxter's nerve neuropathy, tarsal tunnel syndrome, calcaneal bone edema, or pain secondary to biomechanical compensations. [1–3]
Throughout history, this condition has been increasingly well-defined, beginning with Baxter in 1984, who described a complex clinical picture involving recalcitrant plantar fasciitis and Baxter's nerve neuropathy. This was further supported by Bordelon in 1984 and Jorgensen in 1985, who reported similar clinical cases. In the early 21st century, Labib expanded on this by describing a condition comprising plantar fasciitis, tarsal tunnel syndrome, and posterior tibial dysfunction, a finding that was later supported by Odgen's study in 2004. The most recent reference in the literature comes from 2010, when Silvestre Muñoz added calcaneal congestive syndrome to the established conditions of plantar fasciitis and Baxter's neuropathy. [4–7]
The literature on this syndrome highlights several common risk factors in affected individuals, including a sedentary lifestyle, female gender, limited ankle dorsiflexion, excessive pronation of the subtalar joint, and low vitamin D levels. These factors contribute to microfractures in the trabeculae of the calcaneus, leading to the development of the syndrome. [8–10]
Focusing on calcaneal bone edema, or calcaneal congestive syndrome, there is a significant lack of literature on this specific condition as it pertains to the foot. This gap in knowledge leads to a general lack of awareness among healthcare professionals, resulting in underdiagnosis and, consequently, the chronicity of the condition. [7,9]
Calcaneal bone edema can be defined as an increase in fluid with lymphocytic infiltration within the Ward's triangle of the calcaneus, causing disabling pain that predominantly occurs at night. Diagnosis is primarily clinical, typically confirmed with the squeeze test, though fluoroscopy or MRI can be used for corroboration. Its etiology remains unknown, but it is associated with a degenerative bone process, leading to a stress fracture in one of the calcaneal trabeculae, which in turn causes the edema. [2,5,8,11]
The conservative treatment approach, as reported in the literature, involves physical therapy through magnetotherapy or shockwave therapy, as well as vitamin D supplements. However, these treatments are often not curative, necessitating the consideration of invasive methods. The earliest references date back to 1974 when Hassab suggested making 7 to 10 perforations in the lateral cortex of the calcaneus. Subsequent authors, such as Santinini et al. and Seewoonarain et al., advocated for drilling with a 1.8 mm K-wire, either through the lateral or plantar aspect of the calcaneus to avoid damaging any vital structures. In 2020, Rayo et al. proposed performing one or two perforations in the lateral aspect of the calcaneus, followed by aspiration of the clot. [2,8,12–14]
The objective of this article is to determine the pain and quality of life of patients with calcaneal bone edema at 3 and 6 months post-intervention.
Methodology
Data collection for this study was conducted from January 2021 to March 2023. However, due to the low prevalence of the condition, the data collection period was extended until December 2023 to obtain significant data.
An observational, prospective, non-randomized study was conducted with the following criteria [12-14]:
• Inclusion Criteria: Subjects with chronic heel pain lasting more than one year, subjects with previous therapeutic failures, and subjects without a definitive diagnosis.
• Exclusion Criteria: Minors, pregnant women or those with a probability of being pregnant, and subjects with systemic diseases that precluded participation in the study.
A pre-screening was conducted to select subjects based on their suitability for the study. A total of 20 subjects were selected. Once the necessary documentation for participation was provided and the basic medical history was completed, each subject completed the following scales [12-14]:
• Visual Analog Scale (VAS): For pain assessment.
• SF-36 Scale: For quality of life assessment.
• AOFAS Scale: For assessing lower limb function.
These scales were administered at the first consultation and during follow-up visits at 3 and 6 months after the last treatment.
To evaluate the pathology, subjects were asked to undergo a magnetic resonance imaging (MRI) scan of the foot in both coronal and sagittal views to fully visualize the calcaneus in both its longitudinal and transverse axes. Additionally, fluoroscopy was performed to determine the location of the edema, identified by the presence of the double cortical sign [14] (Illustration 1).
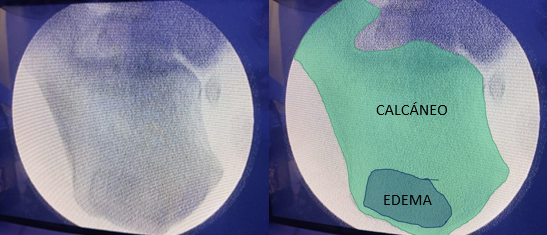
Fluoroscopy of Calcaneal Bone Edema. Source: Own elaboration.
Once a definitive diagnosis of bone edema was confirmed, a clot drainage procedure was performed under local anesthesia on an outpatient basis. This procedure involved making a perforation in the lateral cortex of the calcaneus, precisely in the area corresponding to the edema. After the perforation, a 14G needle was used to aspirate the serohematic contents of the edema (Illustration 2)

Drainage. Source: Own elaboration.
After the procedure, the patient was advised to rest for at least 48 hours and was prescribed oral analgesia (Paracetamol 1g every 8 hours).
After collecting the data for this study, a statistical analysis was performed using Jamovi® version 2.3.26. The results include data related to the general characteristics of the subjects, general biopsychosocial data, examination data, specific data concerning calcaneal bone edema, and specific data on concomitant pathologies.
The data indicate that of the 20 subjects analyzed, 85% were female and 15% were male. These figures are consistent with the typical patient
demographics observed in our clinic, where approximately 75% of patients are women. The average age of the subjects was 57.7 years (SD 9.537). The average height was 1.664 meters (SD 0.072), and the average weight was 77.6 kilograms (SD 11.704).
Regarding the duration of the condition, the average time of progression was 4.95 years (SD 2.139), highlighting the chronic nature of the condition. Notably, 20% of the subjects had a condition lasting either 4 or 6 years.
When analyzing pain (Table 1), the trend showed a significant reduction in pain following treatment, with the average pain score decreasing from 9.1 points before treatment to 0.19 points at 6 months after the final clinical intervention.
| Time Point | Pre-Treatment | 3 Months Post-Treatment | 6 Months Post-Treatment |
| Mean (VAS Score) | 9.1 | 0.95 | 0.19 |
| Sample Standard Deviation | 0.912 | 1.356 | 0.512 |
Table 1: Pain Evolution According to the Visual Analog Scale (VAS). Source: Own data.
| Time Point | Pre-Treatment | 3 Months Post-Treatment | 6 Months Post-Treatment |
| Mean (AOFAS Score) | 20.25 | 60.65 | 89.7 |
| Sample Standard Deviation | 7.893 | 12.857 | 9.895 |
Table 2: Evolution of AOFAS. Source: Own data.
| Time Point | Pre-Treatment | 3 Months Post-Treatment | 6 Months Post-Treatment |
| Mean (SF-36 Score) | 25.1 | 62.35 | 94.35 |
| Sample Standard Deviation | 6.95 | 13.152 | 6.515 |
Table 3: Evolution of SF-36. Source: Own data.
In all subjects of the sample, various tests are conducted to diagnose calcaneal bone edema. In 100% of the cases, the diagnosis is clinical, based on the Squeeze Test, and is accompanied in 35% of cases by fluoroscopy, followed by 30% of cases involving magnetic resonance imaging in coronal and sagittal planes.
Regarding drainage, an average extraction of 9.75 milliliters (SD 5.848) is achieved, with 80
In the year 2000, Dienst M et al. [15] published a clinical case where a patient, after experiencing an axial overload contusion, was diagnosed with bone hematoma in both calcanei via magnetic resonance imaging and bone scintigraphy, following the absence of pathological findings in radiographs and the persistence of the individual's symptoms. This article was the first to reference this clinical entity in the scientific literature and its treatment. Unlike our case series, the treatment was conservative, relying on partial unloading of the left foot (the right foot's symptoms resolved) for approximately 4 months.
Later, in 2003, Santinini S et al. [13] published a study involving 21 patients (25 feet) with chronic heel pain unresponsive to conservative treatment. Although these authors did not refer to the clinical entity of calcaneal bone edema, they noted that patients underwent intervention due to increased uptake on bone scintigraphy. In this instance, as with our patients, surgical treatment was employed, though it involved three microperforations via a medial approach. We, however, used a lateral approach to the lesion out of respect for vascular and nervous structures.
In 2010, Zhou S et al. [16] conducted a study on 50 cadaveric calcanei to analyze the internal microarchitecture of this bone and its relation to fractures occurring within it. Results showed different groups of bone lamellae and, consequently, two potentially weak areas, allowing for the prediction of potential fracture lines. This article shares the zones of bone hypodensity described in our study where calcaneal bone edema is located.
That same year, Thorning C et al. [10] carried out another investigation involving 70 magnetic resonance imaging scans of patients with diabetes and foot ulceration. They concluded that bone marrow edema in the mid and posterior parts of the foot is common in individuals with this pathological condition, although it is usually transient and idiopathic. None of our patients had this condition, but it could be considered an influencing factor in the occurrence of calcaneal bone edema in addition to biomechanical factors.
In 2016, Singh S et al. [9] published a study on the conservative treatment of 18 bone edemas located in the foot, treated with immobilization using a pneumatic boot, either with or without bisphosphonate administration. Good results were obtained at two years of follow-up regarding symptom reduction, though it is noteworthy that only 11% of patients had bone edema in the calcaneus.
In 2018, Hörterer H et al. [17] analyzed the complexity of treating bone edema in the foot and ankle and proposed the possibility of therapy with a prostacyclin analogue, in this case, iloprost, administered intravenously. These authors assessed short- and medium-term results and, although they achieved a 60% reduction in pain and an 80% reduction in bone edema within three months of treatment, they reported minor complications in 12 patients, along with unresolved pain and significant deterioration on magnetic resonance imaging after two years of follow-up.
A year later, Booz C et al. [11] studied virtual reconstruction without calcium via computed tomography compared to magnetic resonance imaging for traumatic calcaneal bone edema. Different radiologists, blinded to the results, analyzed data and images from 62 patients with traumatic calcaneal bone edema, concluding that both quantitative and qualitative analyses of this complementary test showed excellent diagnostic accuracy. This could open a diagnostic pathway for this condition, alongside bone scintigraphy with contrast and magnetic resonance imaging, as demonstrated in our study.
In 2022, Qingwen et al. [18] published an article analyzing calcaneal fractures and their relationship with the internal bone structure. They retrospectively analyzed a total of 226 calcaneal fractures in 210 patients, creating a 3D model from six views of the bone. The study concluded that fracture maps can be created showing recurring patterns of this bone's involvement based on the distribution of its trabecular bone. These maps align, as observed in the previous image, with the most commonly vulnerable areas of the bone described in our study.
In the same year, Chirvi S et al. [19] evaluated the relationship between calcaneal bone density and fractures in 14 cadaveric specimens, concluding that there are significant differences between the bone density of the anterior and posterior regions of the calcaneus. This could help infer the location of fractures in a bone subjected to significant loads. Similarly, our study also shows differences in the intrinsic bone density that predisposes to the location of bone edema in our case.
It is evident that in the scientific literature of the past 20 years, there are few articles published on the diagnosis and management of calcaneal bone edema. Many diagnostic methods and therapies, primarily conservative, are described, leading to controversy in addressing this condition. In our case series, we propose an effective method that significantly reduces symptoms in the short term, allows for a rapid return to normal life for the patient, and respects noble structures (vessels and nerves) by using a lateral surgical approach to the lesion.
There are few studies on calcaneal bone edema, as well as on the quality of life of these patients and its association with other pathologies. This leads to a widespread lack of understanding of the condition, resulting in its underdiagnosis. Therefore, there is a need for a greater number of clinical studies to create high-quality literature on this topic.
The authors declare no conflict of interest.
None.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
