
Mini Review | DOI: https://doi.org/10.31579/2834-5142/011
BSN RN, CDN Renal Nurse Supervisor University of VT Medical Center Burlington, VT 05403.
*Corresponding Author: Peggy Bushey, BSN RN, CDN Renal Nurse Supervisor University of VT Medical Center Burlington, VT 05403.
Citation: Peggy Bushey. (2021) Buttonhole Cannulation of Arteriovenous Fistulas: a Dialysis Nurse's Perspective. International Journal of Clinical Nephrology. 3(1); DOI:10.31579/2834-5142/011
Copyright: © 2021 Peggy Bushey, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 October 2021 | Accepted: 29 October 2021 | Published: 05 November 2021
Keywords: arteriovenous fistulas; trypanophobia; cognitive behavioral therapy
End stage renal disease patients who choose a hemodialysis modality are burdened with the reality that their life is now tied to a dialysis machine between 3- 6 days/week. The impact on their medical, social and psychological well-being is dramatic. One of the biggest fears patients have expressed to us regarding hemodialysis is having to be “stuck with big needles” at each treatment.
The average in-center hemodialysis patient is “stuck with large bore needles” 6 times/week or ~288 times/year barring any “missed sticks” or infiltrations. The home hemodialysis patient increases that number to ~10 x’s/week or ~500 times/yr. Understanding that the average person recoils from the thought of needles, and that ~25% of adults present with a real clinical diagnosis of trypanophobia or “needle phobia” [5], it seems only fitting that we seek out options that would reduce this burden.
Buttonhole cannulation, a technique that entails same site (constant) cannulation of the arteriovenous fistula(AVF) with a blunt needle, offers the patient an alternative to the dreaded “sharp needle stick”. The buttonhole procedure has also been shown to, decrease pain [1], increase the ease of cannulation, be a viable solution to the dilemma of limited cannulation sites, decrease the formation of hematomas [2], and prolong AVF patency [1].
Unfortunately, this technique is also associated with negative outcomes. Same site cannulation leaves a scabbed- over area at the site. Prior to cannulation of this “buttonhole site”, the scab must be completely removed. Incomplete removal of the scab means that the cannulator would be pushing debris containing bacteria into the needle track, causing site infection, and/or into the bloodstream, causing a bloodstream infection (BSI) [5].
In 2007, our in-center hemodialysis units warmly embraced the buttonhole method, and educated all of the dialysis cannulators on this technique. Shortly after initiating this procedure, we noticed an increase in redness at the sites and an increase in BSI’s. At the direction of our medical director, the practice of buttonhole cannulation was discontinued at our in-center facilities.
The home program however, continued the use of this technique with the home hemodialysis patients who had AVFs with resultant few infections. The difference in infection rates was attributed to home patient self-cannulation (or consistent care-partner cannulator) vs. in-center multi-cannulators, and decreased time constraint pressure at home vs. pressure to turn-over patient stations in-center [3]. When a patient did present with an access related infection, we would re-educate the patient and/or care partner to the correct procedure and monitor their progress.
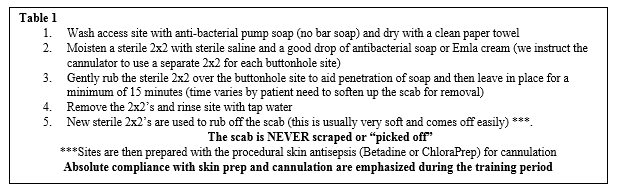
The article “Kinder, Gentler Methods for Scab Removal” “[7] suggested soaking the scabs off rather than the accepted procedure of picking off the scab with tweezers or “pickers” attached to the blunt needles from the manufacturer. We conducted our own “test of change” with a few patients and felt this was indeed, a more acceptable method of site care. Taking this process a step further, developing our current needle site preparation procedure (table 1), we can boast of our positive outcomes.
Since instituting this process, we have had a rare AVF access-related infection (2 infections in 4 years). Investigating each occurrence, revealed an obvious deviation from practice by the patient. In one case the patient washed his arm with the bar soap that was sitting in the sink in his barn, while another patient admitted to “just pushing the scab down into the track”. At the time of update of this article, we have had over 1500 days without an AVF access related infection [4].
All of the patients in our home program who have AVFs are educated on the buttonhole technique. Our Certified Clinical Hemodialysis Technician (CCHT) works one-on-one with each patient/cannulator, usually over a two-week period, to develop the fistula tunnel and guides the patient/cannulator through the steps of successful cannulation. If there are any cannulation issues after the patient goes home, the CCHT will make a home visit to evaluate and re-educate as needed. If it is felt that new buttonholes are required, the patient comes into the clinic for their treatments and we will work with them to initiate the new sites.
The buttonhole technique may not be a viable option for in-center hemodialysis patients, unless they cannulate themselves, due to multiple cannulators, schedule time constraints, and the high probability of missed steps or shortcuts [2]. For home dialysis patients, who are the recipients of ~500 needle sticks per year buttonhole option is a less painful procedure and may be a safe alternative. Strict adherence to the steps outlined in our procedure have proven to be effective in preventing the occurrence of access related infections.
With the proper procedure in place, and a strong patient education program [3], the buttonhole technique is both a viable option and welcome alternative for home hemodialysis patients [4].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
