
Research Article | DOI: https://doi.org/10.31579/2693-7247/217
1 Independent researcher applied pharmacologist, Hospital pharmacist manager, Marijnskaya italy PC area 29121
2 Professor, Department of Medical & Health Sciences for Woman, Peoples University of Medical and Health Sciences for Women, Pakistan
3 Medical laboratory Turin, Citta della salute -Italy
4 YU IMA president RU
*Corresponding Author: Mauro Luisetto, independent researcher applied pharmacologist, Hospital pharmacist manager, Marijnskaya italy PC area 29121.
Citation: Mauro Luisetto, Mashori G.R, Cabianca L, Latyshev O, (2024), Budesonide –Oral Galenic Formulations for Chron Disease, J. Pharmaceutics and Pharmacology Research, 7(11); DOI:10.31579/2693-7247/217
Copyright: © 2024, Mauro Luisetto. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 30 September 2024 | Accepted: 09 October 2024 | Published: 12 November 2024
Keywords: Budesonide; chron’s disease; pediatric, delay release; capsules acido resistance filled with HPMC; metolose; methocel; orals suspension; ready for use veicle ; 3D printing
Aim of this work is to verify the farmaceutical form of oral Budesonide compounded used in Chron’s disease: capsules delay release or oral suspension.
In particular way the kinds of excipients or bases-veicle used in the galenic pharmacy.
The therapeutic need require a release of the API in delayed release.
The Budesonide show low systemic impacts due by its hepatic methabolism vs a tocipal effect useful in this pathology.
Some formulation provided by various pharmacy are reported as well as new technology like the
3D-PRINTING systems for colonic targeting tablets.
Chron ‘s disease can affect both children and adults: as reported in Journal Article Inflammatory bowel disease: The difference between children and adults Judith Kelsen, Robert N. Baldassano Inflammatory Bowel Diseases, October 2008 “Inflammatory bowel disease (IBD) is a group of diseases that include Crohn's disease and ulcerative colitis. Presenting symptoms and therapeutic options are similar in adult and pediatric patients. But there are significant differences in the 2 populations that require separate approaches to treatment and management of the disease in children. IBD is now being recognized with increased frequency in both adults and in children of all ages”
And related the pathology characteristics :
in Mayo Clin Proc. 2017 Jul Crohn Disease: Epidemiology, Diagnosis, and Management Joseph D Feuerstein, Adam S Cheifetz is reported : “Crohn disease is a chronic idiopathic inflammatory bowel disease IBD condition characterized by skip lesions and transmural inflammation that can affect the entire gastrointestinal tract from the mouth to the anus.”
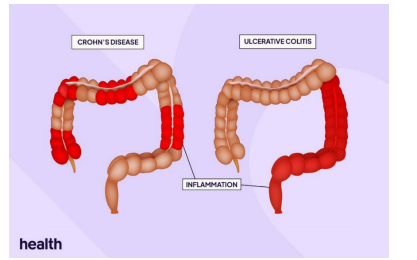
Figure 1: Chron ‘s disease and ulcerative colitis
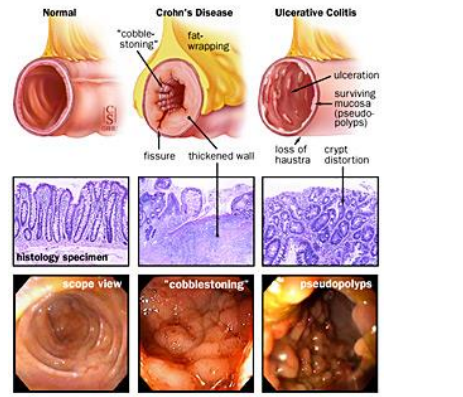
Figure 2: form Jhon Hopkins medicine
And related epidemiology and incindence : In Clin Colon Rectal Surg. 2018 Pediatric and Congenital Colorectal Diseases in the Adult Patient David M. Gourlay, Pediatric Crohn's Disease Daniel von Allmen : “the incidence of Crohn's disease CD in the pediatric population is increasing. While pediatric patients with Crohn's disease exhibit many of the characteristics of older patients, there are important differences in the clinical presentation and course of disease that can impact the clinical decisions made during treatment. The majority of children are diagnosed in the early teen years, but subgroups of very early onset and infantile Crohn's present much earlier and have a unique clinical course” And Between the various therapeutic option before the introduction of the Biological drugs : herap Adv Gastroenterol.2022 A review of the therapeutic management of Crohn’s disease Aditi Kumar, Alexander Cole, Jonathan Segal,and Jimmy K. Limdi “Truelove and Witts first demonstrated the efficacy of corticosteroid treatment in acute severe UC in 1955. Corticosteroids, however, have numerous unwanted side effects, such as metabolic (steroid-induced diabetes, cushingoid appearance, and hepatic steatosis), central nervous system (psychosis, insomnia, and emotional disturbances), gastrointestinal GI (dyspepsia and peptic ulcer), musculoskeletal (osteonecrosis of the jaw and hip, osteoporosis, and growth failure), skin (easy bruising, skin thinning, weight gain, acne, hirsutism, striae, and purpura), and ocular effects (glaucoma and cataracts). Long-term use can also increase the risk of infection, lead to impaired wound healing, and can result in steroid dependence. In 1994, a newer glucocorticoid formulation, budesonide, was shown to have equal efficacy to prednisolone, 16 with a 15 times greater affinity for glucocorticoid receptors, such that 5 mg of budesonide is equivalent to 12 mg of prednisolone. Budesonide has an added advantage of a high first pass liver metabolism and rapid elimination, resulting in minimal systemic absorption and thereby reducing the risk of steroid-induced side effects. “
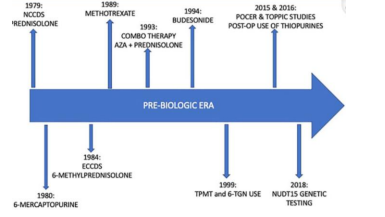
Figure 3: from doi: 10.1177/17562848221078456
Oral Budesonide for Active Crohn's Disease Gordon R. Greenberg et al N Engl J Med 1994 “Budesonide is a corticosteroid with high topical antiinflammatory activity but low systemic activity because of extensive hepatic metabolism”
Related the formulation in use it is possible to see : https://www.bayviewrx.com/formulas/Budesonide-2-mg-10-ml-Oral-Suspension-Asthma-Allergic-Rhinitis-Crohn-s-Disease-Ulcerative-Colitis-Eosinophilic-Esophagitis “The Budesonide 2 mg/10 ml Oral Suspension OS is available in a liquid dosage form. This form allows for the ingredients to be dispersed uniformly throughout a liquid medium, providing a homogeneous mixture for administration. This makes it easy to take and measure the correct dose. It is crucial to take Budesonide exactly as prescribed by your doctor.”
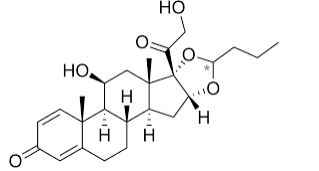
Figure 4: Budesonide - chemical structure formula
Generally the Budesonide Dosage forms can be : oral capsule, extended release (6 mg; 9 mg), oral delayed release capsule (3 mg; 4 mg), oral suspension (2 mg/10 mL), oral tablet, extended release (9 mg) From Mayo clinic : Budesonide in chron’s disease posology: “For oral dosage form (delayed-release capsules): For mild to moderate active Crohn's disease: Adults—9 milligrams (mg) once a day in the morning for up to 8 weeks. Your doctor may adjust your dose as needed. Children 8 to 17 years of age and weighing more than 25 kilograms (kg)—At first, 9 mg once a day in the morning for up to 8 weeks, followed by 6 mg once a day in the morning for 2 weeks. Children younger than 8 years of age or weighing 25 kg or less—Use and dose must be determined by your doctor. For prevention of symptoms of Crohn's disease from coming back: Adults—6 milligrams (mg) once a day in the morning for up to 3 months. Your doctor may adjust your dose as needed. Children—Use and dose must be determined by your doctor” Observing Budesonide Te Arai 3 mg controlled-release capsules technical sheet : in the List of excipients there are : Capsule content Sugar pellets (Maize starch & Sucrose) Ethyl cellulose Dispersion Type B Polysorbate 80 Methacrylic acid polymer type C Triethyl citrate Talc Capsule shell Black iron oxide E172 Red Iron Oxide E172 Titanium dioxide E171 Gelatin
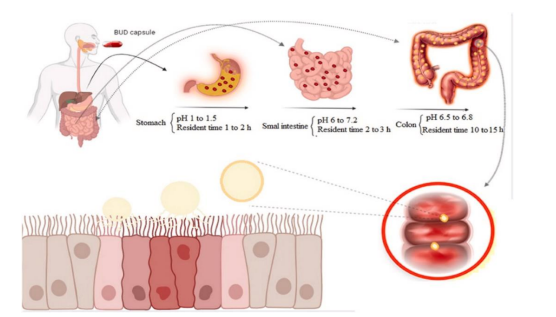
Figure 5: from https://www.pharmaexcipients.com/news/budesonide-second-line/
Therapeutic benefits of budesonide in gastroenterolog Sarah O'Donnell and Colm A. O'Morain https://doi.org/10.1177/20406223103792 “Budesonide is a synthetic steroid of the glucocorticoid family with a high topical antiinflammatory activity. Enteric-coated EC formulations resist gastric-acid degradation, delivering active drug to the small intestine and proximal colon” In https://www.pharmaexcipients.com/news/budesonide-second-line/ “To deliver BUD to the colon, the drug formulation should be formulated so that it prevents the release of the drug in the upper GIT and starts releasing the drug content as soon as it reaches the colon. Various approaches, including the modifying of pharmaceutical formulations using drug delivery systems DDS dependent on microbial degradation, time-dependent and pH-dependent, have been investigated separately or in combination with each other”
Whit an observational method some relevant literature (from 1 to 10) is reported related the topic of this work.
Various figures help better understand the concepts.
An experimental project hypotesys is reported and finally a global consulsion is submitted after analyzing all.
FROM LITERATURE or form professional websites:
https://www.bayviewrx.com/formulas/Budesonide-10-mg-Slow-Release-Acid-Resistant-Capsules-Asthma-Crohn-s-Disease-Ulcerative-Colitis-Allergic-Rhinitis-Eosinophilic-Esophagitis
Budesonide 10 mg Slow Release Acid Resistant Capsules
“Budesonide 10 mg Slow Release Acid Resistant Capsules, formulated with Methocel E4M, are designed to gradually release the active ingredient over an extended period. This controlled-release mechanism offers sustained therapeutic effects, reduces dosing frequency, and improves patient compliance. These capsules are resistant to stomach acid and are used to treat conditions such as Asthma, Crohn's Disease, Ulcerative Colitis, Allergic Rhinitis, and Eosinophilic Esophagitis.
The acid-resistant AR feature of the capsules protects the medication from being degraded in the stomach, thereby enhancing absorption and improving the overall efficacy of the drug. This ensures that the medication is delivered to the site of inflammation in the body, providing relief from symptoms and reducing inflammation.
What is the purpose of the Methocel E4M in the formulation?
Methocel E4M is a type of controlled-release polymer. It is used in the formulation to ensure that the medication is released gradually over an extended period of time. This offers sustained therapeutic effects and reduces the frequency of dosing.” (1)
From Texbook of pharmaceutical excipients ( Fift edition):
“synonyms Benecel MHPC; E464; hydroxypropyl methylcellulose; HPMC; Methocel; methylcellulose propylene glycol ether;methyl hydroxypropylcellulose; Metolose; TylopurIn oral products.
hypromellose is primarily used as a tablet binder,(1) in film-coating,(2–7) and as a matrix for use in extended-release tablet formulations.(8–12) Concentrations between 2% and 5% w/w may be used as a binder in either wet- or dry-granulation processes. High-viscosity grades may be used to retard the release of drugs from a matrix at levels of 10–80% w/w in tablets and capsules” (2)
from a compounding pharmacy service in USA about the BUDESONIDE CPS they provide :
“We put budesonide in an acid resistant capsule, then use a 40% blend of Hydroxypropyl Methylcellulose as a filler to help delay the release of budesonide.”
Tadashi Yokoyama et al
“Primary Assessments. The proportion of patients who achieved remission at week 8 was numerically higher in the budesonide group than in the mesalazine group (30.4 vs. 25.0%; p = 0.526; Fig.reported (3)
Ashish Chopra et al
“Delayed-release budesonide (Entocort EC) is enteric coated and designed to deliver budesonide to the terminal ileum and proximal colon, where Crohn's disease is most common.” (4)
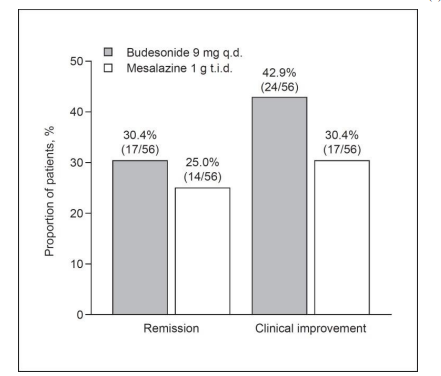
Figure 6: Rates of remission (Crohn's Disease Activity Index [CDAI] score ≤150) and clinical improvement (CDAI score ≤150 or CDAI score decrease from baseline ≥100) at week 8 of the treatment phase. q.d., once daily; t.i.d., three times daily. From Yokoyama et al According Yi Hsuan Ou et al “In this study work , we have demonstrated the ability to engineer 3D printed pill-in-pill (CORR3CT) tablets to target specific sites along the gastrointestinal tract, in particular the colon. The 3D printed tablets are also comparable to commercially available budesonide oral” (5) Rita Cortesi et al “Eudragit®RS microparticles showed a better protection of the drug from gastric acidity than those of Eudragit®RS/Eudragit®RL allowing us to propose Eudragit®RS micro-particles as a hypothetical system of colon specific controlled delivery.”(6) Iborra M et “Budesonide is available in three oral dose forms : a controlled ileal release form, a pH-dependent release formulation, and a MMX formulation. Both controlled ileal and pH-dependent release use enteric coated (Eudragit®, Evonik Industries) pellets and have been approved for treating CD located in the terminal ileum and/or ascending colon. The controlled ileal release form (Entocort®, AstraZeneca, ; Entocir®, Sofar SpA) contains L 100-55 Eudragit® granules, which are resistant to gastric acid degradation and dissolve at pH values above 5.5. A pH-dependent release formulation (Budenofalk®, Dr Falk Pharma) is an enteric coated locally acting glucocorticoid preparation whose pH- and time-dependent coating enables its release into the ileum and ascending colon. This oral formulation consists of a capsule containing L, S, LS, and RS Eudragit® granules that dissolve at pH values above . A new controlled release system, Budesonide MMX® (Cosmo Pharmaceuticals SpA, Lainate, Italy), has recently been developed and researched. MMX technology comprises hydrophilic and lipophilic excipients, both of which are enclosed within a gastroresistant and pH-dependent coating” (7) Jennifer Dressman et al “ Prolonged (extended) release of budesonide is ensured by embedding the drug in a multimatrix (MMX) formulation” (8)
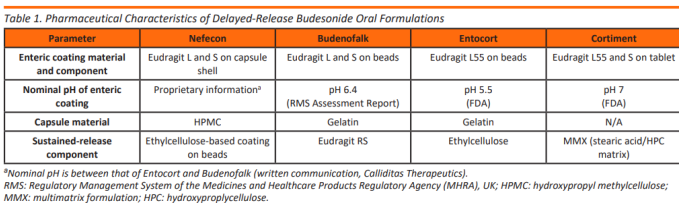
Figure 7: from doi.org/10.14227/DT300423P224
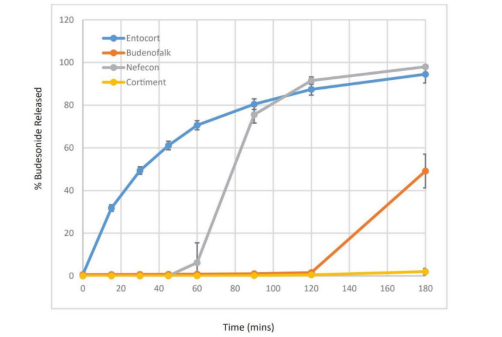
Figure 8: From J. Dressman Comparative Dissolution of Budesonide from Four Commercially Available Products for Oral Administration
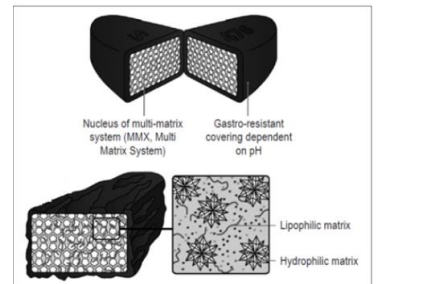
Figure 9: from https://tasnimpharma.com/mmx-technology/
Fouad S. Moghrabi et al “To date, several enteric, ready-to-fill capsules are commercially available, which claim to prevent gastric drug release. These include: Bio-VXR® (BioCaps) with an undisclosed formulation of vegetable capsules, DRcapTM (Lonza Capsules and Health Ingredients) nutraceutical capsules composed of HPMC and gellan, designed to swell and delay disintegration, enTrinsicTM drug delivery capsules (Lonza) composed of cellulose acetate phthalate (CAP) and Vcaps® Enteric capsules (Lonza) composed of HPMC, HPMC-AS polymers and gellan gum as the gelling agent . In 2021, EUDRACAPTM (Evonik, Darmstadt) HPMC capsules coated with methacrylic acid copolymers that can easily be opened and closed were launched .”(9) To be observed in nutraceutical setting also : from Extended Release of Vitamin C Matrix Tablets with TYLOPUR Xtend Nutra@ “WLOPUR Xtend Nutra@ is an excellent choice as a highly compressible, hydrophilic matrix agent for nutraceutical and nutritional tablet applications. Straight forward and easy direct compression formulation of extended rèlease hydrophilic matrix tablets of natural active compounds (Vitamic C used here as an example)using TYLOPUR Xtend Nutra@ is cost effective. The results show that TYLOPUR Xtend Nutra@ regulates the release of Vitamin C in a controlled manner, slowing it signifìcantly depending on the amount used”. (10)
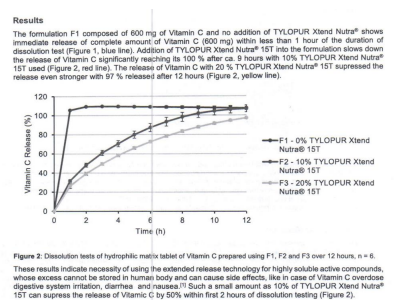
Figure 10
To verify the efficiency of the use of AR CPS filled with API mixed in Methocel E4M (40 %) is needed
To test the level of the API after 1-2 h in acid environment Ph similar to gastric fluids and after a buffered
Medium like intestinal PH.
If the system tested really protect the gastro sensible API the matrix methods can be used for this scope.
Budesonide is currently used in therapy of Chron’s disease or other inflamatory condition.
This kind of cortison show low systemic toxiciy and good topic efficacy: this due by and extensive liver methabolism.
Various strategies are used by the producers to provide a delayed release to ptotect from gastric fluids degradation: kind of capsules, enteric coating of the capsules, matrix systems (ex hydroxipropilcellulose based).
In current therapy various are the formulation available : form capules slow - delay release – acido resitence Or also in oral supension.
Interesting the cps AR filled with the API in Methocel E4M (about 40%) a controlled-release polymer used by some pharmacy .
It is fundamental for the therapy of chron’s disease with BUDESONIDE to use an delayed release
Oral pharmaceutical form in order to protect form the gastric acid PH.
(Generally The registered drugs are gastroresistance pellets inside normal capsules )
Various are the formulation used : of interest the use of AR CPS filled with Methocel 40% to delay the release of the API in the intestinal setting and the oral suspension ( as versatile pharmaceutical form)
NO
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
